























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

TRILLIANT HEALTH RESEARCH
Research
Timely trend analysis. Free in your inbox.
Receive weekly studies from Trilliant Health.
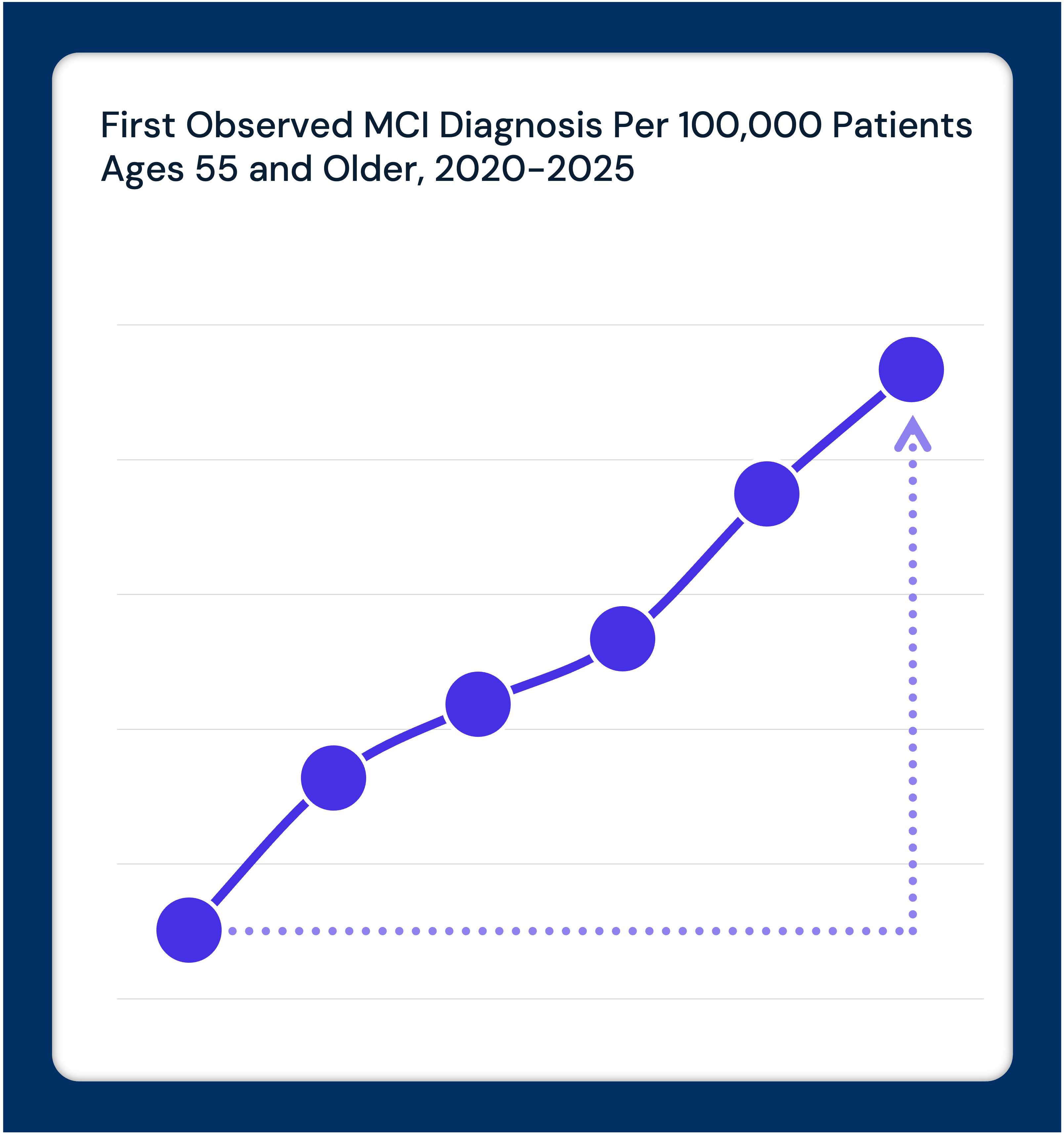
With Blood-Based Test Approval, Alzheimer’s Biomarker Testing Has Grown 37.5x, and Dementia Diagnosing Has Shifted Toward Earlier, Milder Stages
Read the StudyJuly 30, 2026
With Blood-Based Test Approval, Alzheimer’s Biomarker Testing Has Grown 37.5x, and Dementia Diagnosing Has Shifted Toward Earlier, Milder Stages
Biomarker tests for Alzheimer’s increased 37.5x between 2023 and 2025, diagnoses trended milder, but specialist shortages may leave the health system unprepared for surging dementia care demand.
Jessica Brantez • Allison Roberts, Ph.D. • Katie Patton • Allison Oakes, Ph.D.
StudiesJuly 23, 2026
Commercial Negotiated Rates for Cancer-Related Procedures Are Increasing Faster than CPI in the Majority of U.S. Markets
Commercial rates for cancer procedures outpaced national CPI in more than half of U.S. markets between 2024 and 2026 – exposing risks for self-funded employer benefit planning.
Katie Patton • Maura Eshleman • Jim Browne • Allison Oakes, Ph.D.
StudiesJuly 16, 2026
Pharmacy Utilization Management Expands as Nearly Half of Initially Rejected Prescriptions Go Unfilled
Only 54% of branded prescriptions initially rejected by prior authorization were ultimately approved in 2024, with Medicaid beneficiaries facing lower approval rates.
Katie Patton
StudiesJuly 09, 2026
One in Four Cancer Patients Had an Emergency Department Visit with a Nonspecific Finding Prior to Diagnosis, and Nearly 1/3 Waited More Than 180 Days for Confirmation
Nearly one in four cancer patients had a nonspecific ED visit before diagnosis. Delays ranged from 31-123 by cancer type, with repeat ED visits – not outpatient follow-up – as the most common next step.
Katie Patton • Austin Miller • Jessica Brantez
StudiesJuly 02, 2026
High Medicare Dependence and Low Overall Margins Leave Rural Hospitals Most Vulnerable to Pending Program Expiration
Rural hospitals face the lowest margins and serve older, sicker populations, leaving them vulnerable as the Medicare-Dependent Hospital Federal program nears expiration.
Clara Petrucelli • Katie Patton
StudiesJune 25, 2026
Most Internal Medicine Residents Continue to Specialize Amid Growing Gaps in Primary and Geriatric Care
Internal medicine residents increasingly subspecialize, favoring high-paying fields. Geriatric, infectious disease and palliative fellowships go unfilled amid a worsening physician shortage.
Katie Patton • sam-hall
StudiesJune 18, 2026
GLP-1 Patients Without Preexisting Gastrointestinal Disorders Had Higher Rates of Gastrointestinal Events Than the General Population
GLP-1 patients without prior GI disorders had higher rates of GI events and inpatient surgeries than the general population, with 65% continuing GLP-1 therapy post-surgery.
Katie Patton • Austin Miller
StudiesJune 11, 2026
More Than Half of GLP-1 Patients Have a Diagnosis Associated with a Newly Approved or Investigational Indication
More than half of GLP-1 patients have a diagnosis tied to an emerging or newly approved indication, with obstructive sleep apnea and depression being the top co-occurrences.
Katie Patton • Austin Miller
StudiesJune 04, 2026
Episode Cost and Quality Are Not Correlated Across Hospitals Subject to Mandatory LEJR Bundled Payment Under TEAM and Proposed CJR-X
There is no observable correlation (r=-0.1) between LEJR episode cost and quality across hospitals subject to TEAM and the proposed CJR-X model.
Katie Patton • David Taylor
Interested in citing our research? Please follow this guide.
