






















Featured Study
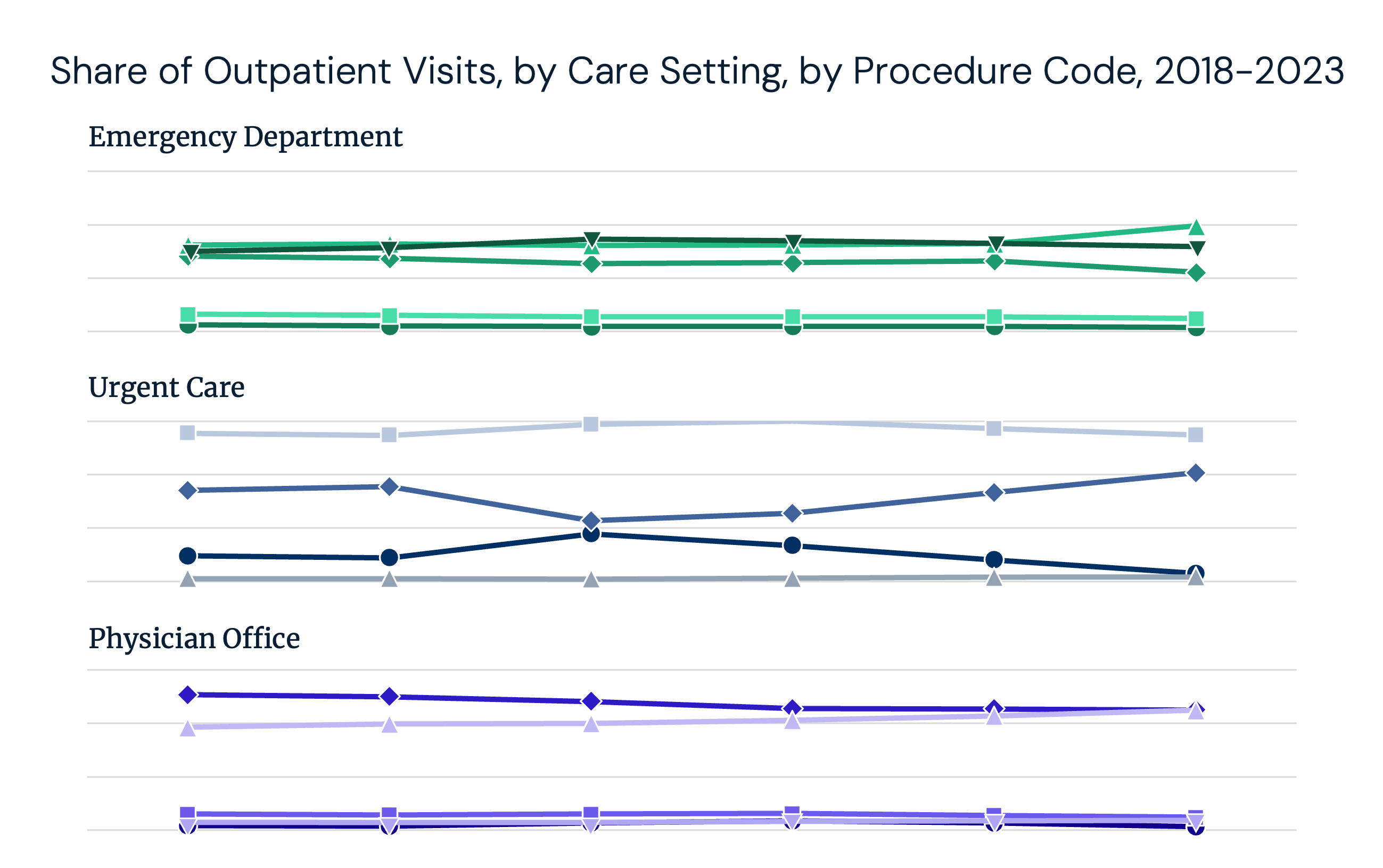
Changes in Coding Intensity Suggest HowUpcodingIs Happening Across Outpatient Settings
A measurable trend toward higher-acuity billing across several settings of care has raised concerns about “upcoding” – the implications of which extend beyond payer reimbursements.
Health economy trends.
Free in your inbox.
Track health economy trends with research from Trilliant Health’s research team.
Changes in Coding Intensity Across Outpatient Settings
Read the Study
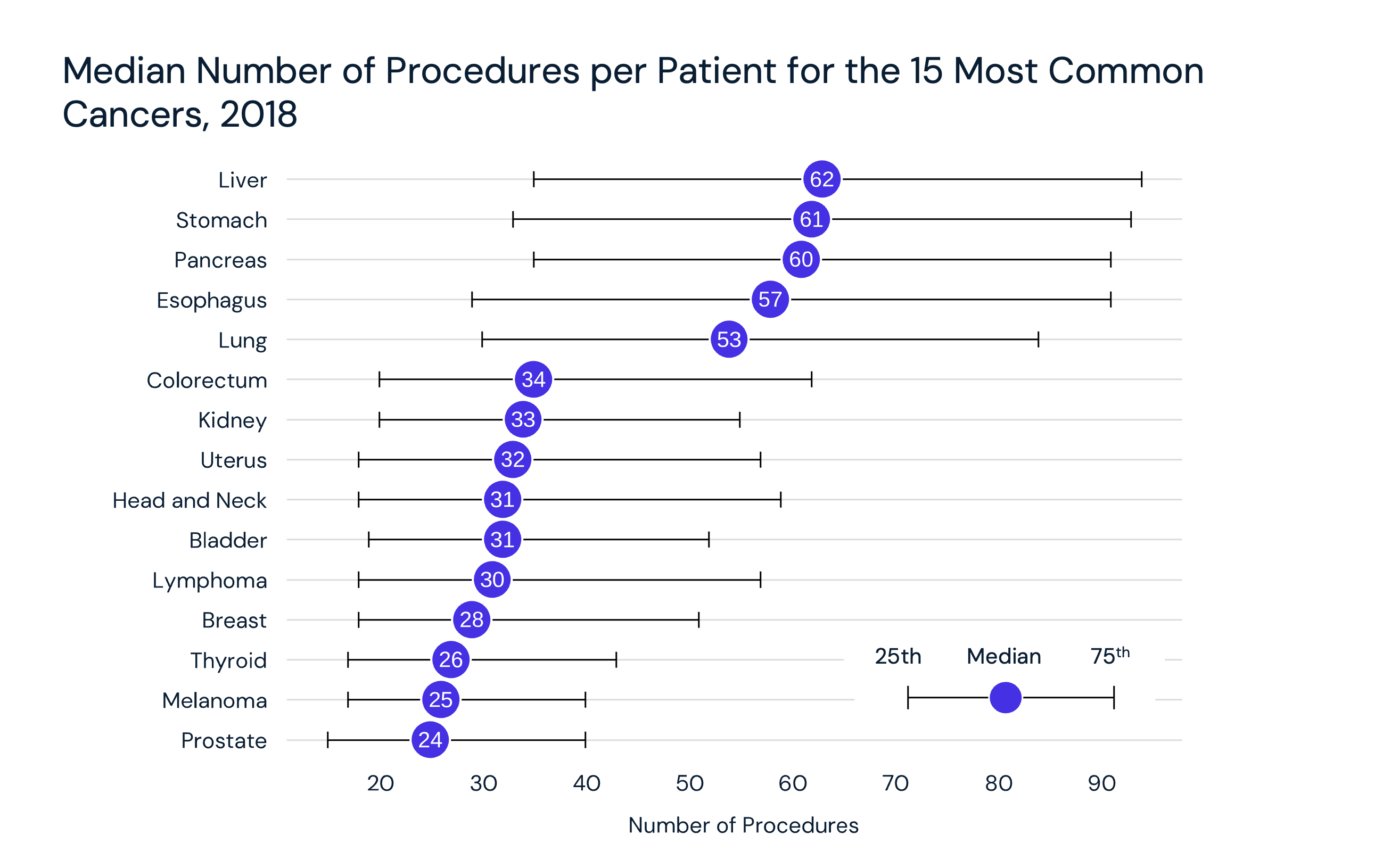
Outpatient Utilization Rates in Cancer Care Reflect Procedure-Specific Shifts
Read the Study

The 24 Data Stories That Defined 2024
Read the Study

2024 Trends Report Conclusion: Health Economy Stakeholders Who Focus on Value Optimization Will Establish a Competitive Advantage
Read the Study

Trend 8 of 8: Employers Are Better Equipped To Demand Value for Money
Read the Study
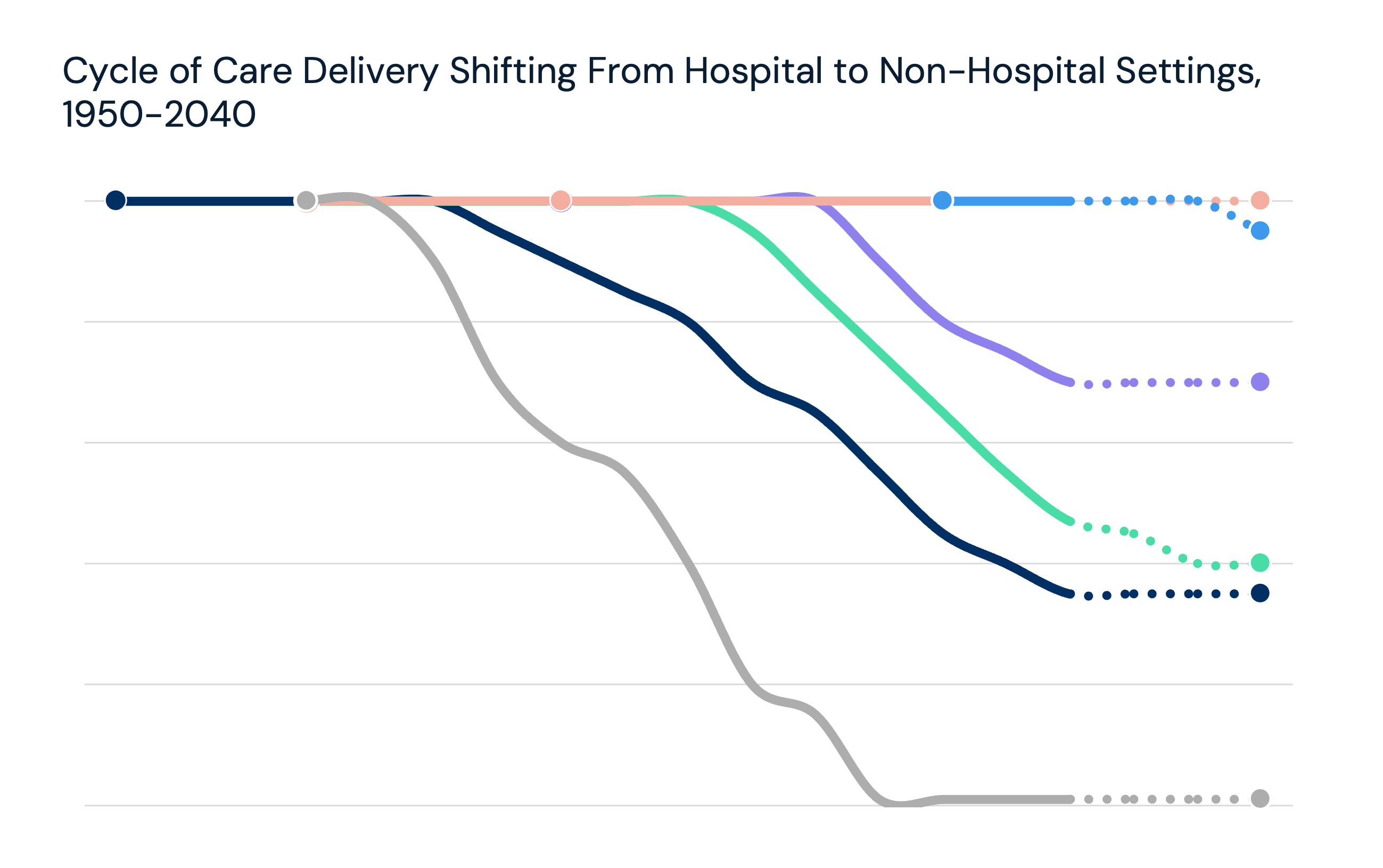
Trend 7 of 8: Lower-Cost Care Settings Can Offer Better Value
Read the Study
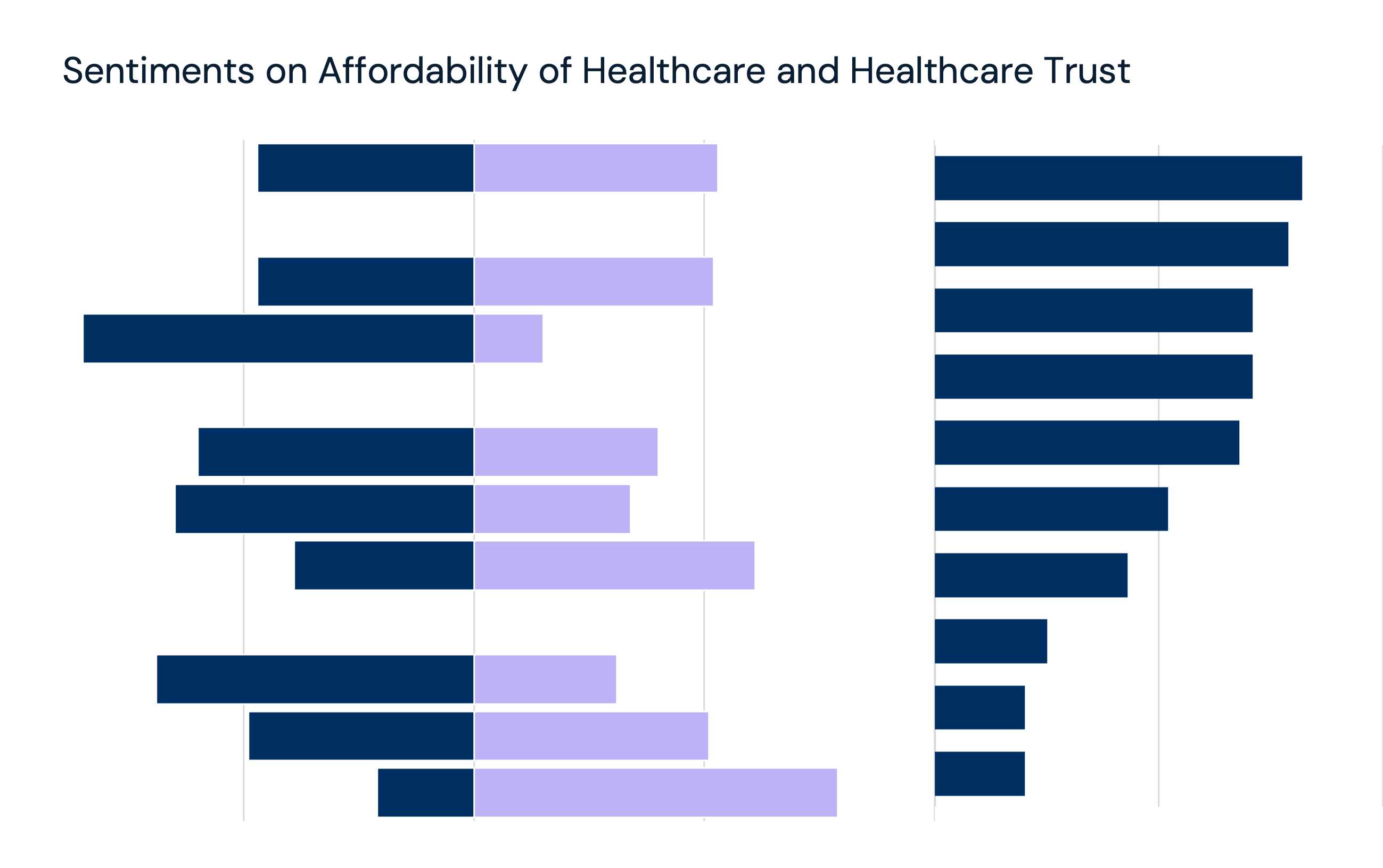
Trend 6 of 8: Forced Consumerism Due to Cost Shifting Has Fostered Fragmentation Without Corresponding Value
Read the Study
Trend 5 of 8: Supply Constraints Are Correlated With Inadequate Yield
Read the Study
Trend 4 of 8: The Value of Technological Advancements Is Uncertain
Read the Study
Interested in citing our research? Please follow this guide.
