























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Key Takeaways
-
GLP-1s have the potential to revolutionize clinical treatment of obesity and diabetes, but current utilization patterns of GLP-1s are not correlated with clinical disease, primarily because of off-label use.
-
In New York City, prescribing of GLP-1s is concentrated in the Upper East Side neighborhood with 231.3 patients per 10K individuals, but only a quarter of this population has a recorded type 2 diabetes diagnosis.
-
Of the patients prescribed GLP-1s in New York City, 43.8% do not have a recorded type 2 diabetes diagnosis. The non-diabetes population skews younger, is 74.7% female and is 90.6% commercially insured.
The unprecedented demand for prescription drugs, specifically GLP-1 receptor agonists (GLP-1s), for type 2 diabetes and obesity has gained significant attention. Given abundant media coverage of these drugs, persistent off-label use and supply shortages, we examined GLP-1 use in a densely populated and diverse geographic area—New York City.
Background
GLP-1s have been used for nearly two decades to treat type 2 diabetes.1 Sold by Novo Nordisk under the brand names Ozempic®, Wegovy® and Rybelsus® and by Eli Lilly under the brand name Mounjaro®, these drugs have been in short supply for months. Most notably, off-label use of Ozempic®, which is solely indicated for type 2 diabetes, for weight loss has grown increasingly common.2
Our prior research revealed a substantial increase in the number of patients prescribed drugs like Ozempic® and Mounjaro®. Patient volumes for GLP-1s more than tripled between Q1 2020 and Q3 2022, yet only 57.0% of these patients had an official type 2 diabetes diagnosis.3 Without insurance, GLP-1s can cost between $892 to $1,300+ per month, and insurers are far less likely to reimburse the cost of drugs prescribed for off-label use.4
The unknown long-term side effects of off-label GLP-1s, high cost per treatment and supply challenges could have serious implications for all healthcare stakeholders. Thus, analyzing patient demographics and the extent of both on-label and off-label use is needed. Additionally, it is useful to understand these trends within a major market like New York City, as opposed to the national level alone. Intra-market variation, especially for such a financially and demographically diverse area, reveals trends likely impacting the entire U.S. market.
Analytic Approach
Leveraging national all-payer medical and pharmacy claims data, we examined prescription volumes for three GLP-1s, Ozempic®, Wegovy® and Mounjaro®, across 34 New York City neighborhoods in 2022. For each neighborhood, we identified the number of patients with GLP-1 activity per 10K individuals, the proportion with a type 2 diabetes diagnosis and select patient demographics (i.e., age, gender, insurance source).
Findings
In New York City, 56.2% of patients prescribed a GLP-1 have a documented type 2 diabetes diagnosis. Among these patients who both take a GLP-1 and have diabetes, the average age is 59.2, and 73.5% are commercially insured. In contrast, patients prescribed this medication without a type 2 diabetes diagnosis are younger (average age of 47.5), more likely to be commercially insured (90.6%) and female (74.7%).
At the neighborhood level, the highest rate of GLP-1 utilization was in Upper East Side/Gramercy with 231.3 patients per 10K individuals (Figure 1). Within that population, 67.8% were female, the average patient age was 49.6 and 26.6% had type 2 diabetes. Conversely, the East New York/New Lots neighborhood had the lowest GLP-1 utilization rate of 121.3 per 10K individuals. Within that population, the average patient age was 53.5 and a higher proportion (74.2%) had diabetes.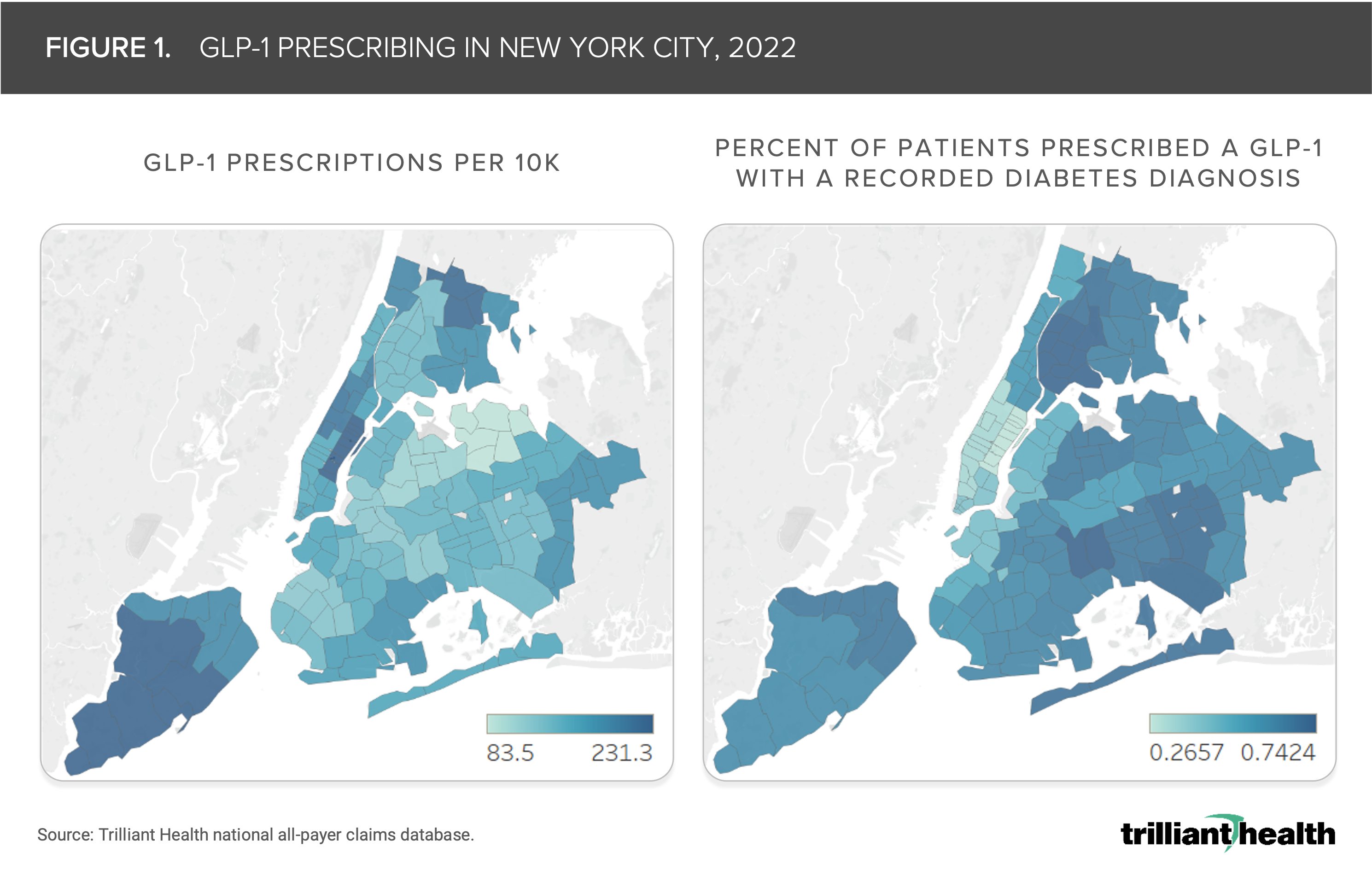
The mismatch between clinical indication and demand for GLP-1s in New York City is primarily attributable to off-label use (i.e., utilization by patients without Type 2 diabetes). The Upper East Side neighborhood has one of the highest life expectancies and the lowest rates of diabetes and obesity in New York City, and yet prescriptions for GLP-1s are concentrated in that neighborhood. 5,6 However, in East New York, which has one of the highest obesity rates in New York City, GLP-1 prescribing rates are lower than more affluent neighborhoods and are more concentrated among patients with a type 2 diabetes diagnosis.7
GLP-1s have the potential to transform the way obesity and diabetes are treated. The long-term effects of off-label use of GLP-1 medications for non-obese younger adult patients without type 2 diabetes remain unclear. However, heightened demand is resulting in lack of supply for patients who meet the clinical indications for these drugs. Moreover, increasing supply to meet demand (including off-label) may not be sufficient in making these medications available for high-need patients. Will adjusting prescribing patterns to regulate demand for patients with clinical indication ensure appropriate access?
As health plans—both public and private—analyze and revise coverage arrangements for GLP-1s, it is critical to understand the demographics of patients currently prescribed these medications. As healthcare spending approaches 20% of U.S. GDP, increased demand for an expensive drug used by many for non-clinically indicated weight loss is likely to have a profound impact on healthcare expenditures, health equity and the overall health status of American patients.
To learn more, please see a recent article from The New York Times that featured our study findings.
Get the latest insights delivered to your inbox.
Related Research
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
