























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
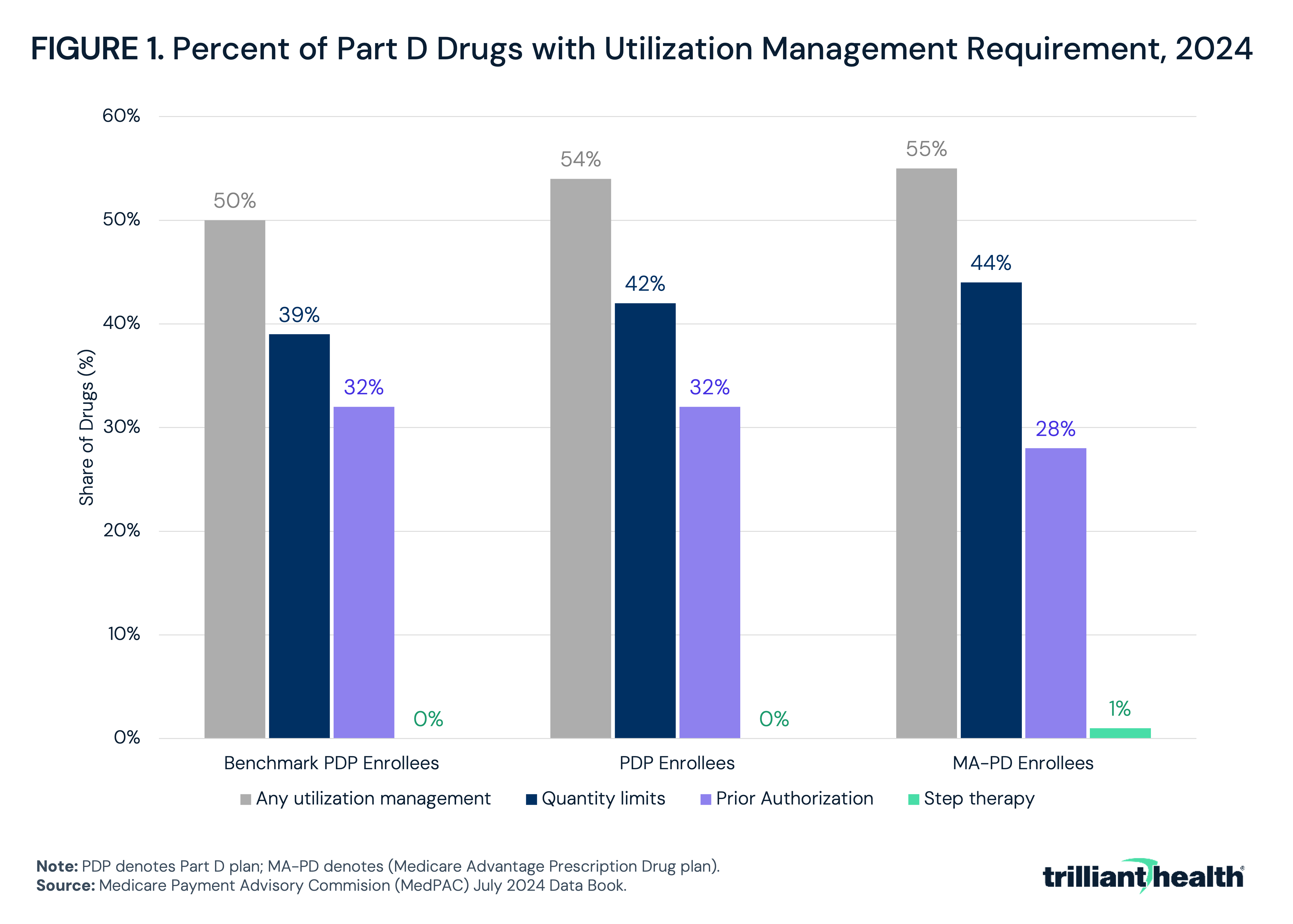
- In 2024, half of Part D drugs were subject to some form of utilization management, with minimal variation between plan types.
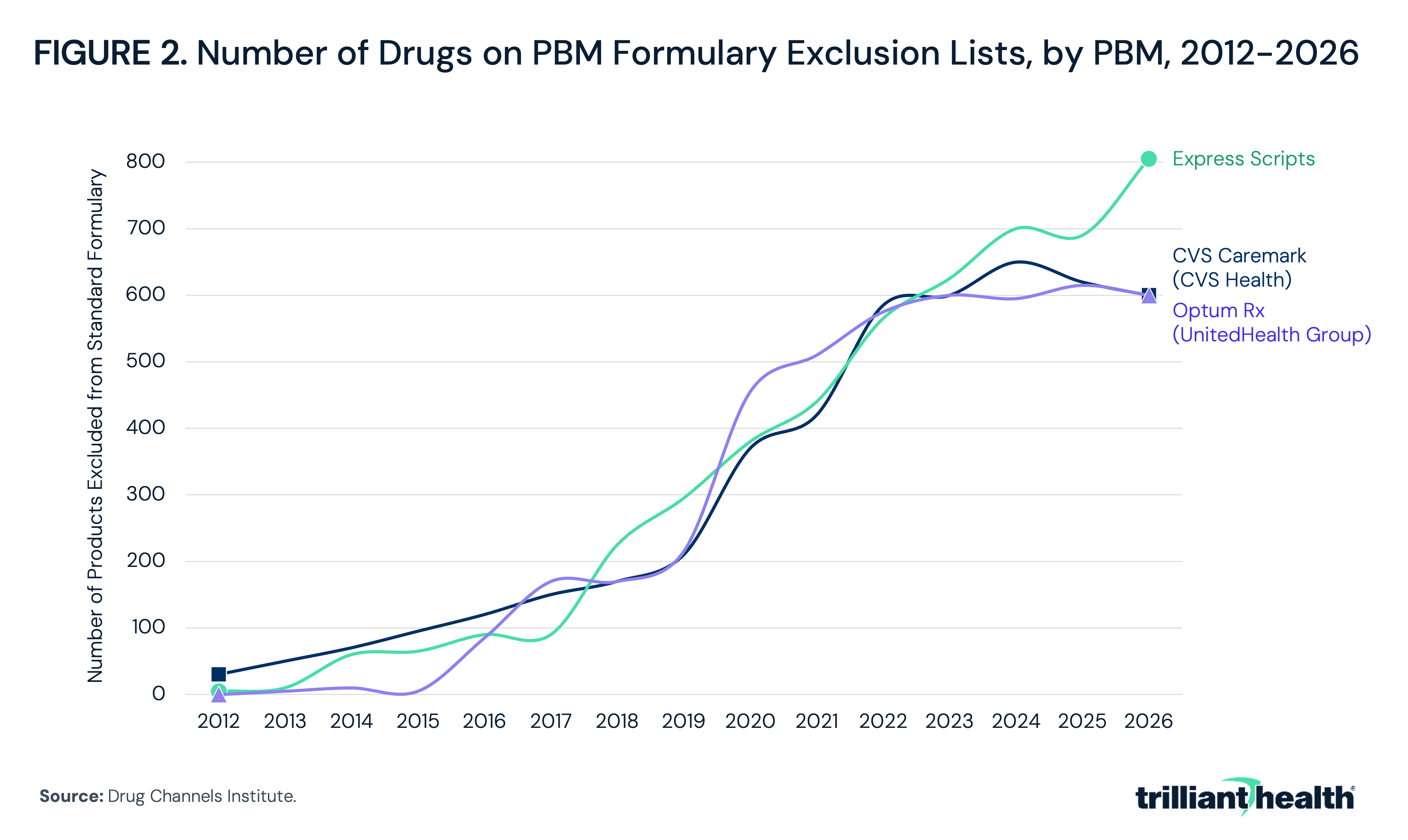
- The standard formulary exclusion lists of the three largest PBMs – which collectively process nearly 80% of U.S. prescriptions – have each grown to more than 600 products.
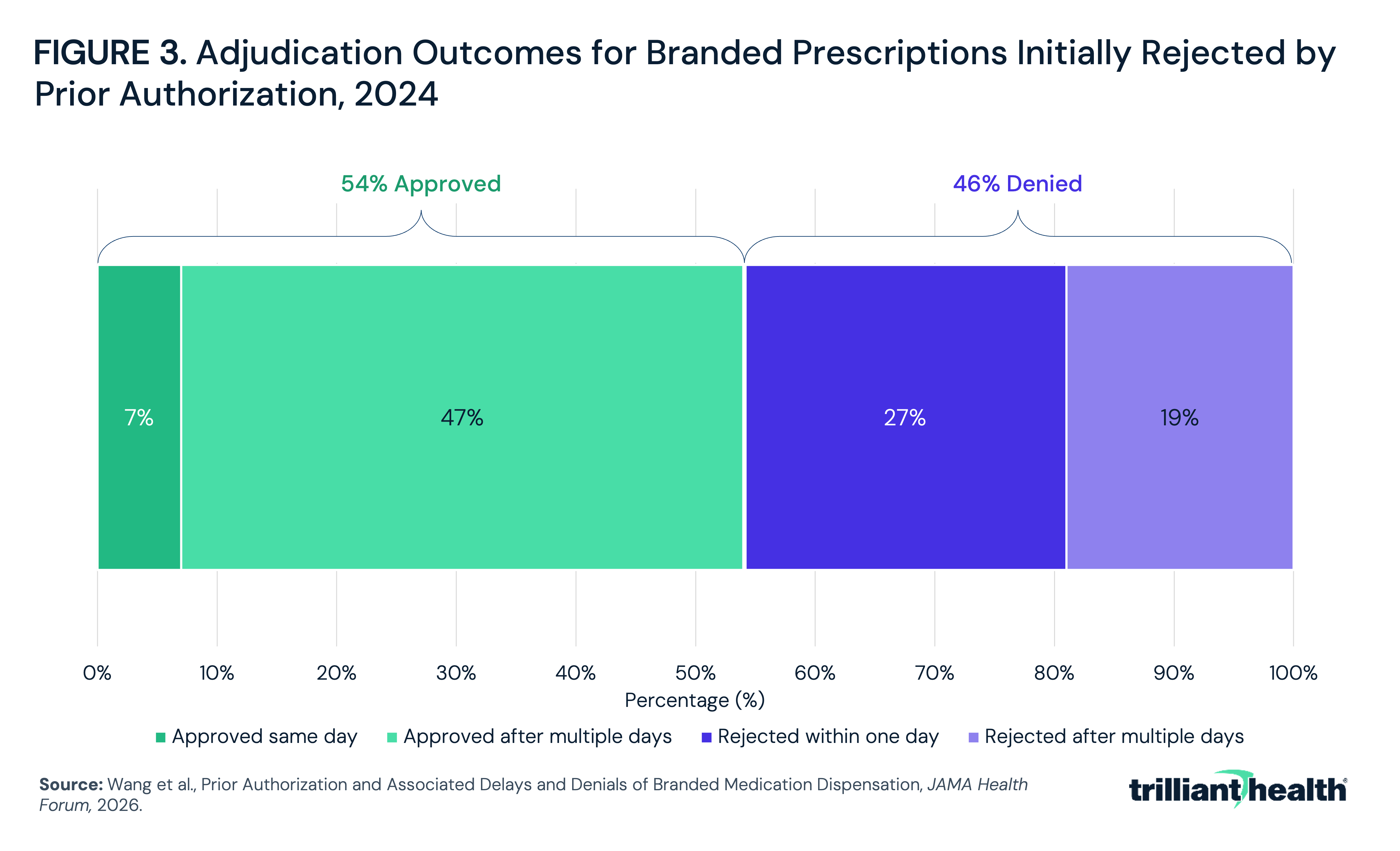
- Transaction-level evidence shows that among branded prescriptions initially rejected by prior authorization in 2024, only 54% were ultimately approved.
Retail prescription drug spending reached $467.0B in 2024, increasing 7.9% from 2023, and CMS projects it will be the fastest-growing major category of national health expenditures over the next decade.1,2 Beyond negotiating prices, payers rely on utilization management (UM) to constrain drug spending. UM is generally implemented and managed by pharmacy benefit managers (PBMs), the companies that administer prescription drug benefits on behalf of health plans, employers and other payers by designing formularies, negotiating manufacturer rebates and processing pharmacy claims.3 Prior authorization and step therapy are the dominant forms of UM. These requirements often determine which medications patients receive and when they receive them, regardless of what a prescriber has ordered.
The existence of prior authorization suggests that a material percentage of healthcare diagnostics, therapeutics and procedures are not necessary (i.e., they require external assessment to determine if they represent low-value care or even waste). That reality is reinforced by the fact that the United States lacks a regulatory body or an industry framework to measure healthcare value, whether generically at the intersection of cost and quality or specifically in terms of quality-adjusted life years (QALYs). As a result, America’s exorbitant healthcare costs have compelled health economy stakeholders to constrain spending through alternative measures, such as UM. Recently, Federal regulation and voluntary payer commitments have started to reshape prior authorization with respect to medical benefits. However, attention to the application of UM for pharmacy benefits is comparatively limited.
Background
Prior authorization and step therapy are the dominant forms of pharmacy UM in the U.S. health economy, and both are utilized to promote guideline-concordant prescribing and constrain spending on high-cost therapies (e.g., GLP-1 agonists). Prior authorization requires prescriber-submitted clinical justification before a health plan will cover a medication. Step therapy requires patients to try and fail a preferred alternative first. Preferred status is typically based on lower cost, though rebate incentives can also influence formulary placement. Along with quantity limits and formulary exclusion, both methods are managed primarily by PBMs on behalf of health plan sponsors.
Two-thirds of new drugs approved from 2013 to 2017 and covered in Medicare Part D required prior authorization from at least one large insurer, with 40% of those drugs subject to prior authorization criteria more restrictive than their FDA label.4 Additionally, researchers found step therapy applied in 38.9% of specialty drug coverage policies across 17 large commercial plans, with 55.6% of protocols more stringent than corresponding clinical guidelines and only 34.0% consistent with them.5 Research suggests pharmacy UM can yield net savings. One analysis of Medicare Part D found that prior authorization reduced use of targeted drugs by 26.8% and lowered drug spending by $96 per beneficiary-year against roughly $10 in administrative costs, with affected patients split evenly between those redirected to a related drug and those who did not fill a prescription.6 The American Medical Association's most recent physician survey, which spans prior authorization for both prescription medications and medical services, found practices complete an average of 40 prior authorizations per physician per week, accounting for 13 hours of physician and staff time.7 In the same survey, 95% of physicians reported that prior authorization delays access to necessary care, and 79% reported that patients abandon treatment because of authorization challenges, reflecting persistent physician objection to requirements that can override a prescriber's clinical judgment.
Whether pharmacy UM reduces costs is different from whether it creates value. It is well established that prescription adherence is a prerequisite for a quality outcome from a pharmaceutical intervention, and a prescription fill is required for adherence. A KFF survey found 16% of insured adults incurred delays or denials related to prior authorization, and a separate analysis found prescription drug denials by private insurers increased 25% from 2016 to 2023.8,9 A study in the Journal of Clinical Oncology found that when Part D plans imposed new prior authorization requirements on oral anticancer drugs, patients already stable on a therapy experienced an average 10-day delay in prescription fills with increased odds of discontinuation within 120 days.10 When UM disrupts fills for patients already established on a therapy, any near-term savings come with the possibility of disease progression, higher-acuity care and worse outcomes downstream.
The evidence is clear that UM creates administrative friction, which can lead to delayed treatment for patients and has become a major bipartisan policy issue. The CMS Interoperability and Prior Authorization final rule, which as of January 1, 2026, requires Medicare Advantage, Medicaid, CHIP and Marketplace payers to render expedited prior authorization decisions within 72 hours and implement electronic prior authorization application programming interfaces (APIs) by 2027, does not apply to drugs.11,12 Likewise, this effort does not seek to make pharmacy UM more transparent. At the state level, at least 29 states have enacted step therapy override or PA reform statutes, though none can regulate the self-funded employer plans that cover approximately 100M Americans. Any attempt to compel self-funded employers to comply with pharmacy UM reform would require Congress to amend the Employee Retirement Income Security Act (ERISA), a change that has little support, presumably because self-funded employers are increasingly focused on limiting the growth of the pharmacy benefit.13,14
This analysis examines how extensively pharmacy UM is applied, how its use has changed over time and what its expansion means for patients' access to prescribed medications.
Analytic Approach
Using published research and industry data, this study examines trends in the prevalence, outcomes and regulation of pharmaceutical prior authorization and step therapy, including Medicare Part D formulary restrictions, the growth of PBM formulary exclusions and prior authorization adjudication outcomes.
Findings
In 2024, 50% of Part D drugs and 54% of Part D plan (PDP) enrollees were subject to some form of UM, with 42% of enrollees subject to quantity limits and 32% to prior authorization (Figure 1).
The standard formulary exclusion lists from each of the three largest PBMs – which collectively process nearly 80% of U.S. prescriptions – have grown to more than 600 products (Figure 2). While the pace of growth has slowed in recent years, the exclusion lists have expanded from a narrow set of brand-name drugs with generic equivalents to include biosimilars, specialty therapies and oncology medications.
A 2026 JAMA Health Forum all-payer analysis of 205,896 branded prescriptions initially rejected by prior authorization found that only 35% were adjudicated the same day, with just 7% approved on the day of the patient's first fill attempt. The remainder required a median of six days to resolve, and only 54% were ultimately approved (Figure 3). Within the same analysis, approval rates were lowest for Medicaid beneficiaries (48%, vs. 60% in Medicare), and prescriptions for patients with multiple chronic conditions were most likely to be delayed. Among the 10 most-dispensed molecules in the sample, tirzepatide (i.e., Mounjaro® and Zepbound®) had the lowest approval rate at 49%.
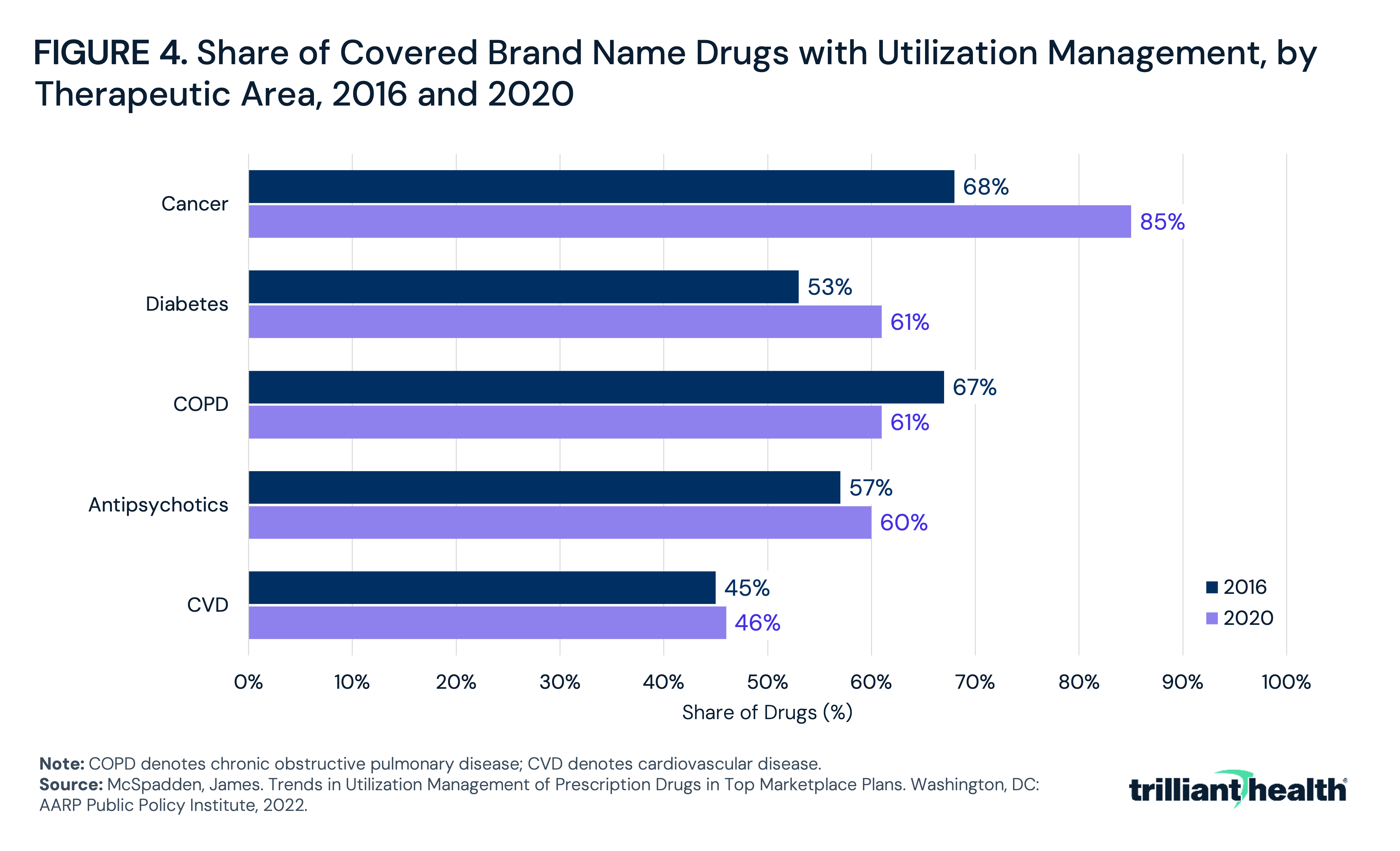
UM is applied unevenly across therapeutic areas. An analysis of the top 10 Marketplace plans in each state found that the share of covered brand name cancer drugs subject to utilization management increased from 68% in 2016 to 85% in 2020, the largest increase among the five therapeutic areas examined (Figure 4). Diabetes drugs increased from 53% to 61% over the same period, while antipsychotic and cardiovascular drugs were roughly unchanged, and COPD drugs declined from 67% to 61%.
Conclusion
Pharmacy UM is no longer a targeted intervention applied to exceptional therapies but rather is increasingly utilized for most branded medications, first through formulary exclusion, followed by prior authorization. In a health economy where pharmacy spending is disproportionately driven by high-cost therapies with list prices frequently exceeding $1,000 per month, payers and employers have legitimate reasons to manage utilization. Even so, the increasing use of formulary exclusion for biosimilars calls into question whether UM is a tactic to steer volume toward a PBM-affiliated private-label product or to preserve rebate arrangements rather than to control utilization of an inherently high-cost therapy.15,16
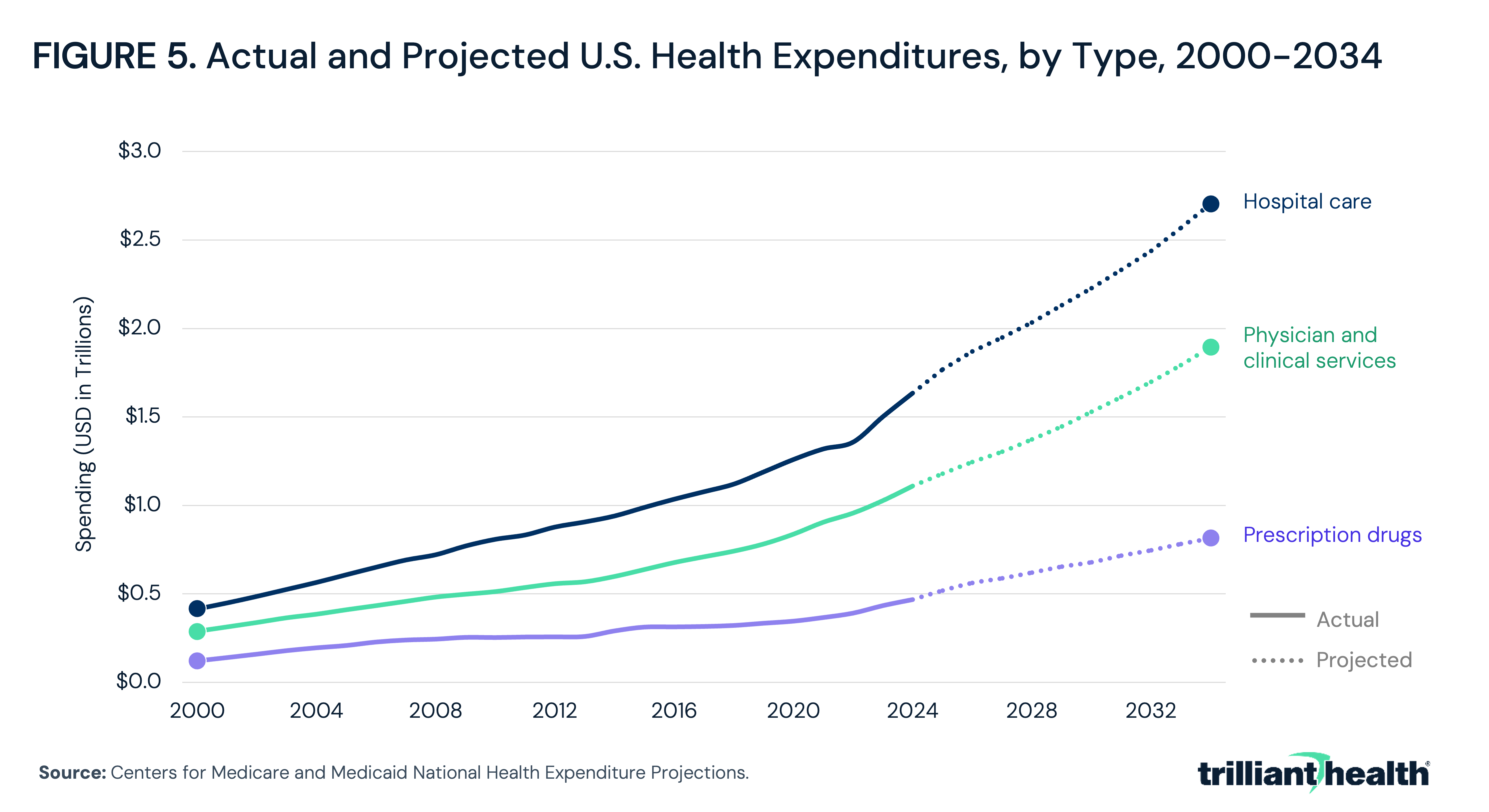
Policymakers are rightly focused on the rate of increase in hospital spending, which is the largest sector of the U.S. health economy. Even so, based on CMS projections, prescription drug spending is projected to grow faster than both hospital and physician care between 2024 and 2034, 74.4% compared to 65.5% and 70.9%, respectively (Figure 5). As a result, the primary focus of Federal reforms of UM for the medical benefit to the exclusion of the pharmacy benefit raises questions.
In theory, the purpose of a formulary is to curate a list of efficacious drugs, while the purpose of UM is to curate the most cost-effective of those efficacious drugs. From that perspective, UM should be binary – approve the most cost-effective and clinically efficacious drugs 100% of the time and deny any non-clinically efficacious drugs 100% of the time. Such an outcome would be the closest the U.S. health economy could come to value for money in pharmaceutical spend since the U.S. does not prioritize using QALYs as a formulary standard. Notably, UM is focused on utilization to the exclusion of interventions related to price, which could reduce spending without impacting access.
The reality of UM is different from the theory, and the fact that 46% of denials resulting from some form of pharmacy UM are sustained suggests a formulary problem. Whether that formulary problem originates in FDA approvals that put into conflict by the substantial portion of FDA’s funding that comes from those it regulates, or it arises from the inscrutable nature of PBMs is a question for Congress. And, from a constitutional perspective, the cost problem that pharmacy UM attempts to solve originates wholly in patent law protections, an enumerated power of Congress under Article I, Section 8.
The barriers erected by pharmacy UM are clearly effective in reducing drug spending, but reducing cost by restricting or denying access does not guarantee a systemic cost reduction. The administrative reviews of prescription refills and step therapy can and do impact patients, whether by delaying or interrupting treatment. Less obvious is the value for money accruing to society from pharmacy UM, both for the drugs that are approved and those that are denied. That pharmacy UM results in denial of 46% of prescriptions undoubtedly means one of two things: either that an FDA-approved therapy is not, in fact, fit for purpose or, alternatively, that some number of Americans do not receive potentially life-changing or life-preserving therapies. The fact that denials result from “black box” decision models influenced by opaque financial incentives is even more concerning.
In response to rising hospital costs, Federal policymakers have exerted significant effort to make hospital prices transparent, one result of which is now that every hospital rate is freely and easily accessible. However, the historic lack of price transparency never prevented an American from receiving treatment in a hospital emergency department. In contrast, Federal policymakers have yet to force price transparency on PBMs, whose refusal to approve prescribed therapies has undoubtedly cost more than one American his or her life.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
