























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
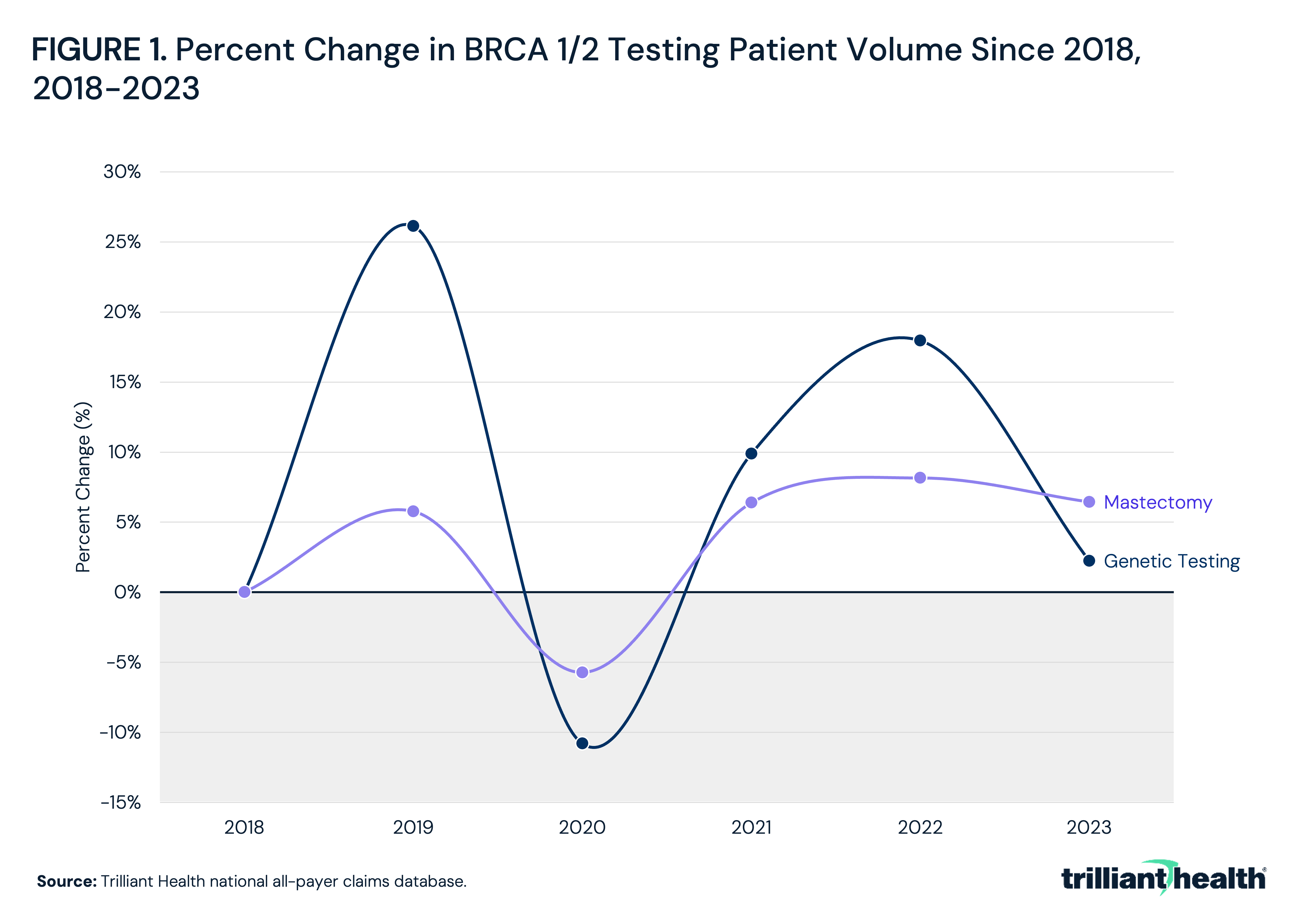
- BRCA1/2 genetic testing volume increased by 26.1% from 2018 to 2019 and 18.0% from 2018 to 2022.
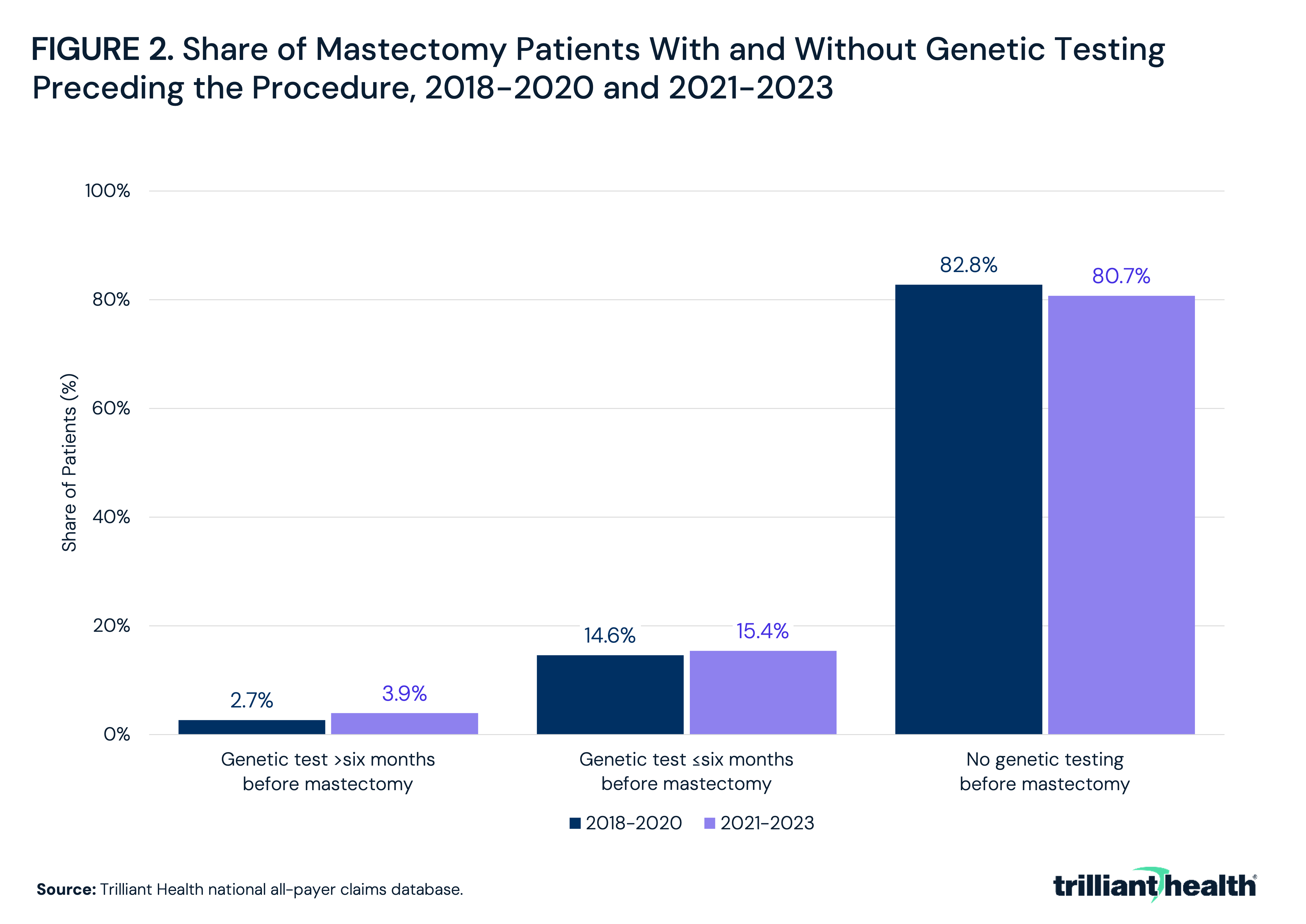
- Most mastectomy patients did not receive genetic testing prior to surgery, though this share increased from 17.2% in 2018-2020 to 19.3% in 2021-2023.
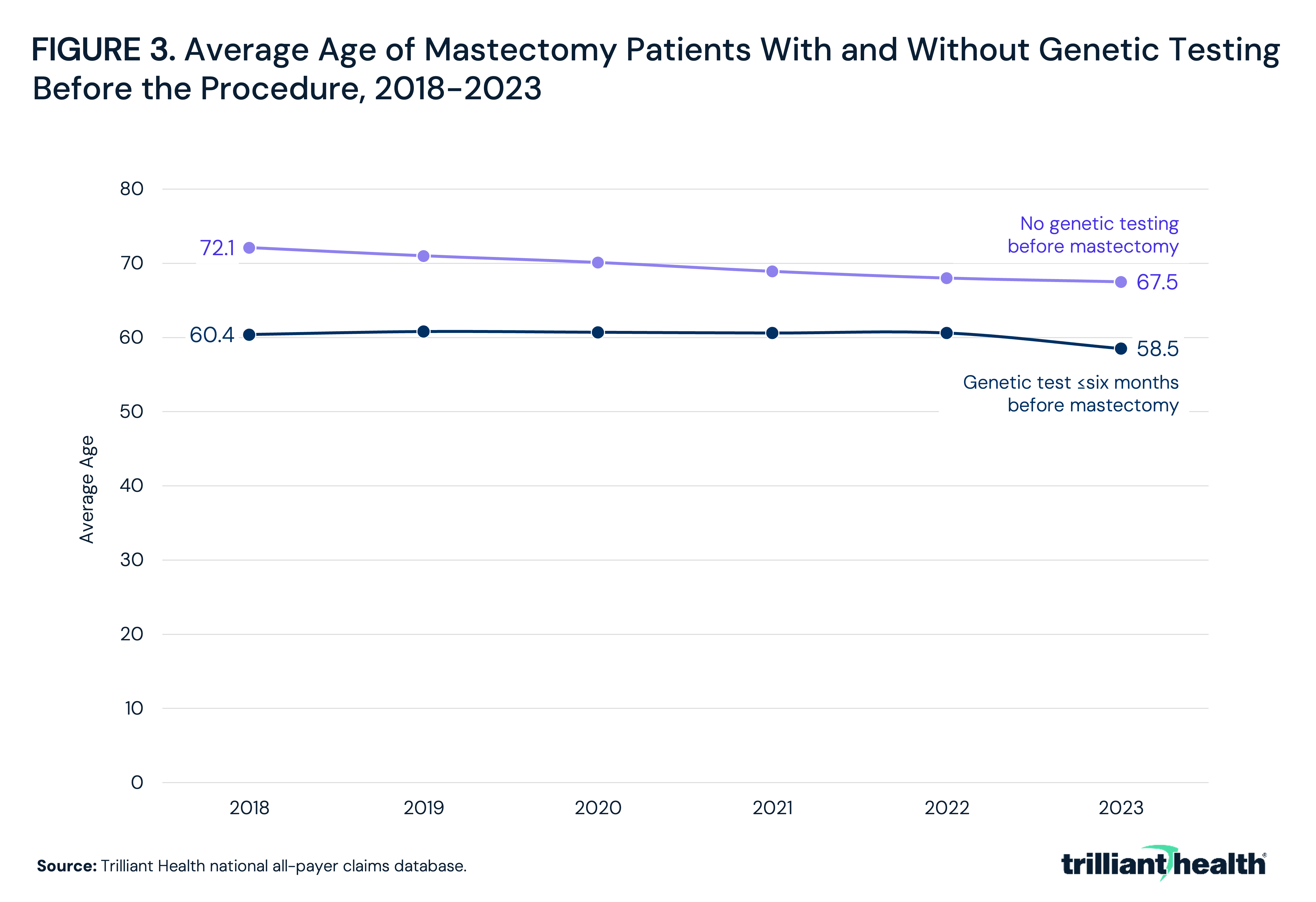
- Mastectomy patients without genetic testing were consistently older, with average age declining from 72.1 in 2018 to 67.5 in 2023.
Advances in genetic testing, including multigene panels and direct-to-consumer (DTC) options, have expanded the availability of risk information across populations, enabling patients and clinicians to engage in more proactive screening and preventive decision-making. Genetic testing is a foundational tool for personalized medicine, offering a one-time assessment to inform lifelong screening strategies, preventive interventions and downstream treatment decisions. Within the broader context of genetic testing expansion, BRCA1/2 (BReast CAncer gene) testing represents a high-evidence, guideline-driven use case, identifying individuals at substantially elevated risk for breast and ovarian cancer.
Mastectomy provides a clinically meaningful lens to study the downstream implications of genetic risk identification. While most patients undergo mastectomy following a confirmed malignancy, others pursue preventive surgery in the absence of a formal diagnosis, often informed by BRCA1/2 and multigene panel testing or elevated risk profiles. This analysis characterizes mastectomy patient journeys – both for patients with and without formal breast cancer diagnoses and those with and without receipt of genetic testing.
Background
Genetic testing has expanded substantially in recent years, driven by increasing awareness of hereditary risk, broader integration into clinical care and the emergence of DTC testing options. A growing number of companies now offer testing outside traditional care settings, which contributes to increased access and corresponding demand, even among individuals without a high-risk medical history. This expansion reflects a broader shift toward earlier risk identification and prevention, with the potential to inform screening decisions and prophylactic action before disease onset. Expanded access to genetic testing presents both the opportunity for early detection but also the potential for over-screening and false positives.
Breast cancer serves as a relevant example for analyzing genetic testing upstream from interventional care. It is the most common cancer among women in the United States, with an estimated 270,000 women diagnosed and 42,000 women dying from the disease annually.1 Established U.S. Preventive Services Task Force (USPSTF) guidelines emphasize routine mammography beginning at age 40, with earlier and more intensive screening recommended for high-risk populations, including those with a family history or known genetic predisposition.2 Insurance coverage expansion has reinforced these recommendations.
USPSTF guidelines recommend risk assessment, genetic counseling and BRCA1/2 testing for women with relevant personal or family history, and these services are generally covered without cost-sharing for eligible patients. BRCA testing has been clinically available since the mid-1990s and was incorporated into USPSTF guidelines in the early 2000s. Still, BRCA testing remains underutilized, and coverage remains variable for downstream interventions such as prophylactic surgery – especially for women not meeting the high-risk criteria.3 Differences across payer types, prior authorization requirements and documentation of medical necessity influence whether and when patients receive testing and treatment. This is despite the fact that women with a BRCA1/2 mutation carry a 45-65% lifetime risk of developing cancer, versus 7% in the general population.4 For these patients, clinical guidelines often recommend enhanced surveillance, chemoprevention or prophylactic surgery, including bilateral mastectomy, which can reduce breast cancer risk by up to 85-100%.
Within the broader expansion of genetic testing, BRCA testing represents a high-evidence, guideline-driven use case that is often delivered within insurance coverage arrangements, making it a useful bellwether for understanding how genetic risk identification influences downstream clinical decisions such as surgery.5 Patients with confirmed cancer diagnoses may undergo surgery as part of standard treatment, with or without prior genetic testing. In contrast, patients without a cancer diagnosis may pursue mastectomy following genetic testing, representing a fundamentally different clinical pathway. Understanding trends in genetic testing is critical to understanding the evolving nature of prevention, early diagnosis and treatment.
Analytic Approach
National all-payer claims were leveraged to identify patients receiving BRCA1/2 genetic testing between 2018 and 2023. Among patients receiving mastectomies, rates of BRCA1/2 genetic testing preceding the mastectomy were examined. Rates of pre-mastectomy genetic testing were compared between two time periods: 2018 to 2020 versus 2021 to 2023. Average patient age was also examined.
Findings
From 2018 to 2023, percent changes in BRCA1/2 genetic testing patient volume varied year to year but generally increased. Relative to the 2018 baseline, genetic testing volume increased by 26.1% in 2019, declined by 10.8% in 2020 and subsequently increased by 9.9% in 2021, 18.0% in 2022 and 2.2% in 2023 (Figure 1).
Across both time periods, 2018-2020 and 2021-2023, the majority of mastectomy patients did not receive genetic testing prior to the procedure, though there were slight increases in testing utilization. Among all mastectomy patients, the share with prior genetic testing increased from 17.2% in 2018-2020 to 19.3% in 2021-2023 (Figure 2). More specifically, the share of all mastectomy patients receiving genetic testing within six months prior to mastectomy increased from 14.6% to 15.4%, while testing more than six months prior increased from 2.7% to 3.9%.
From 2018 to 2023, the average age of mastectomy patients varied by genetic testing status but showed a similar decline over time. Patients tested within six months prior to mastectomy had an average age of 60.4 in 2018, which declined to 58.5 in 2023 (Figure 3). Patients without genetic testing prior to mastectomy were older across all years, with average age decreasing from 72.1 in 2018 to 67.5 in 2023.
Conclusion
Mastectomy patient journeys are increasingly stratified by access to and timing of genetic testing, with implications for both clinical appropriateness and resource utilization. While genetic testing volume has grown rapidly, the majority of patients still undergo surgery without prior testing, indicating both expansion and incomplete integration of genetic testing into surgical decision-making pathways. These patterns suggest missed opportunities for risk-informed decision-making.
These findings should be interpreted through the lens of BRCA1/2 genetic testing as a high-value clinical tool. When applied appropriately, one-time genetic testing allows for the earlier identification of high-risk individuals and the use of preventive or less invasive interventions that may ultimately improve patient care and health outcomes while reducing spending. In this context, the relatively low rate of pre-surgical BRCA testing may represent under-realization of a high-impact, evidence-based test.
BRCA1/2 genetic testing is just one example in a rapidly evolving field where an expanding catalog of hereditary cancer panels, polygenic risk scores and tumor-based genomic assays are reshaping how patients are screened, counseled and treated. As the clinical applications of genetic testing broaden, insurance coverage policy will be a primary determinant of whether these advances translate into meaningful changes to diagnosis and treatment. Realizing the full value of genetic testing will depend not only on continued innovation, but also on ensuring appropriate access and alignment with evidence-based guidelines.
BRCA testing represents a high-value application of genetic screening due to its strong evidence base, well-defined risk thresholds and clear linkage to clinical action, including enhanced surveillance and prophylactic surgery. This direct connection between test results and intervention distinguishes it from many newer genetic and genomic tests. Many emerging screening modalities, including multi-cancer early detection tests such as those developed by GRAIL (Galleri®), have more limited evidence on clinical utility and downstream impact, with recent studies raising questions around false positives, overdiagnosis and the potential for unnecessary follow-up care.6 Additionally, a recent prospective clinical trial using the Galleri® test was temporarily put on hold, likely due to poor clinical performance.7 Despite this, these tests are increasingly utilized by patients outside of traditional insurance and physician arrangements. For example, Galleri® can be requested directly through the company's website via an independent telemedicine provider or through Function Health with a list price of $949. Notably, most health insurance plans do not currently cover Galleri® – meaning patients are largely self-pay.8
As genetic testing continues to expand, maintaining high evidentiary standards and ensuring that utilization is aligned to clinical value will be critical to avoiding unintended increases in low-value testing and associated low-value care cascades. At the same time, enabling broader and more consistent use of high-value tests like BRCA1/2 represents a significant opportunity for early disease detection and reduced system-wide spending.
In the near future, the implications of genetic testing's expanding role extend well beyond oncology. Across cardiology, neurology and reproductive medicine, genetic and genomic information is increasingly shaping preventive strategies and treatment selection. As genetic testing becomes more deeply embedded across medicine, its influence on high-stakes decisions will only grow. Ensuring that this influence is evidence-based, clinically integrated, and equitably distributed will be essential not only to optimizing individual patient outcomes, but to preserving the integrity of care delivery more broadly.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
