























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
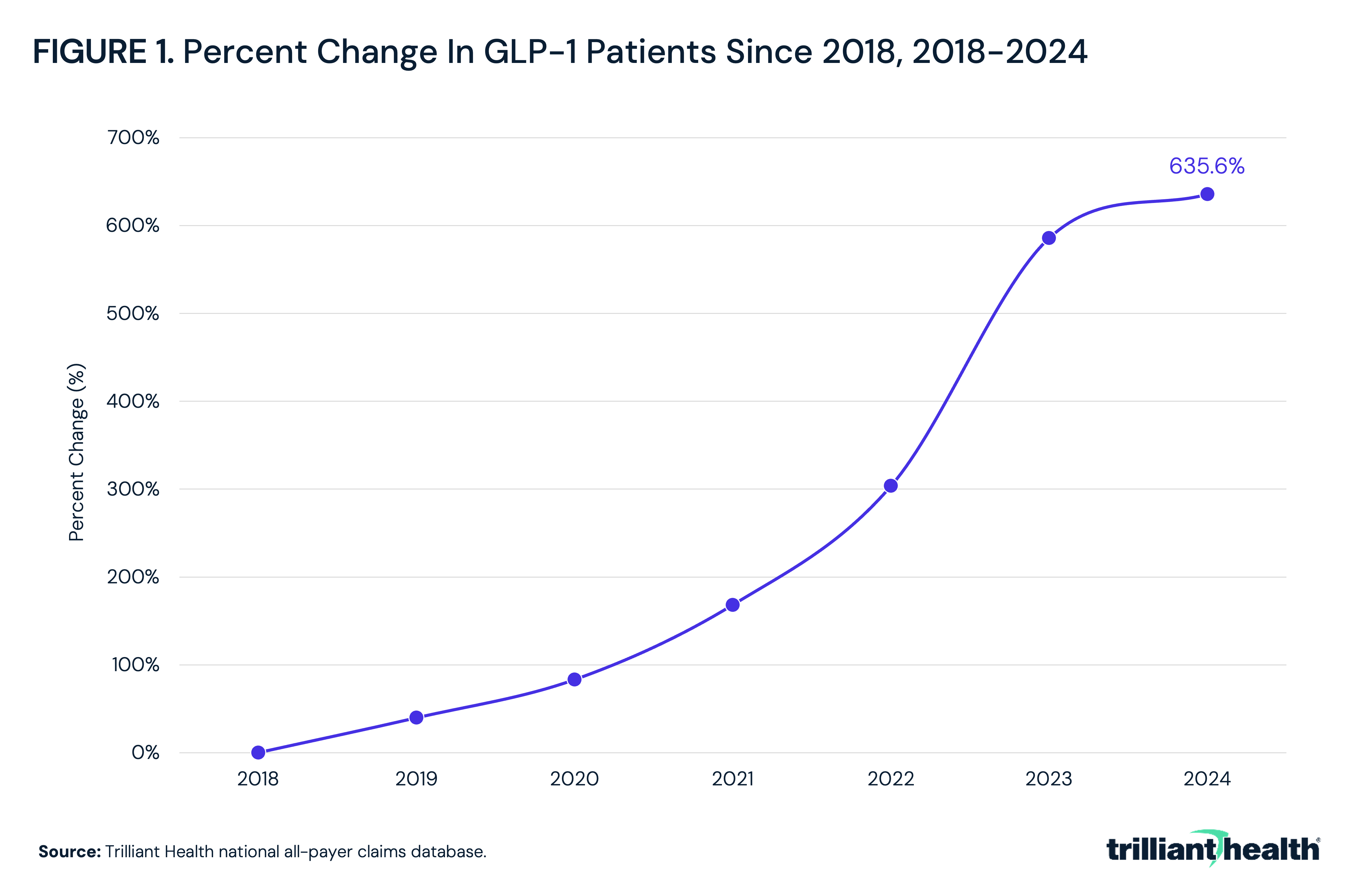
- The number of patients on GLP-1 receptor agonist therapies increased by 635.6% from 2018 to 2024, with the steepest growth between 2021 and 2023.
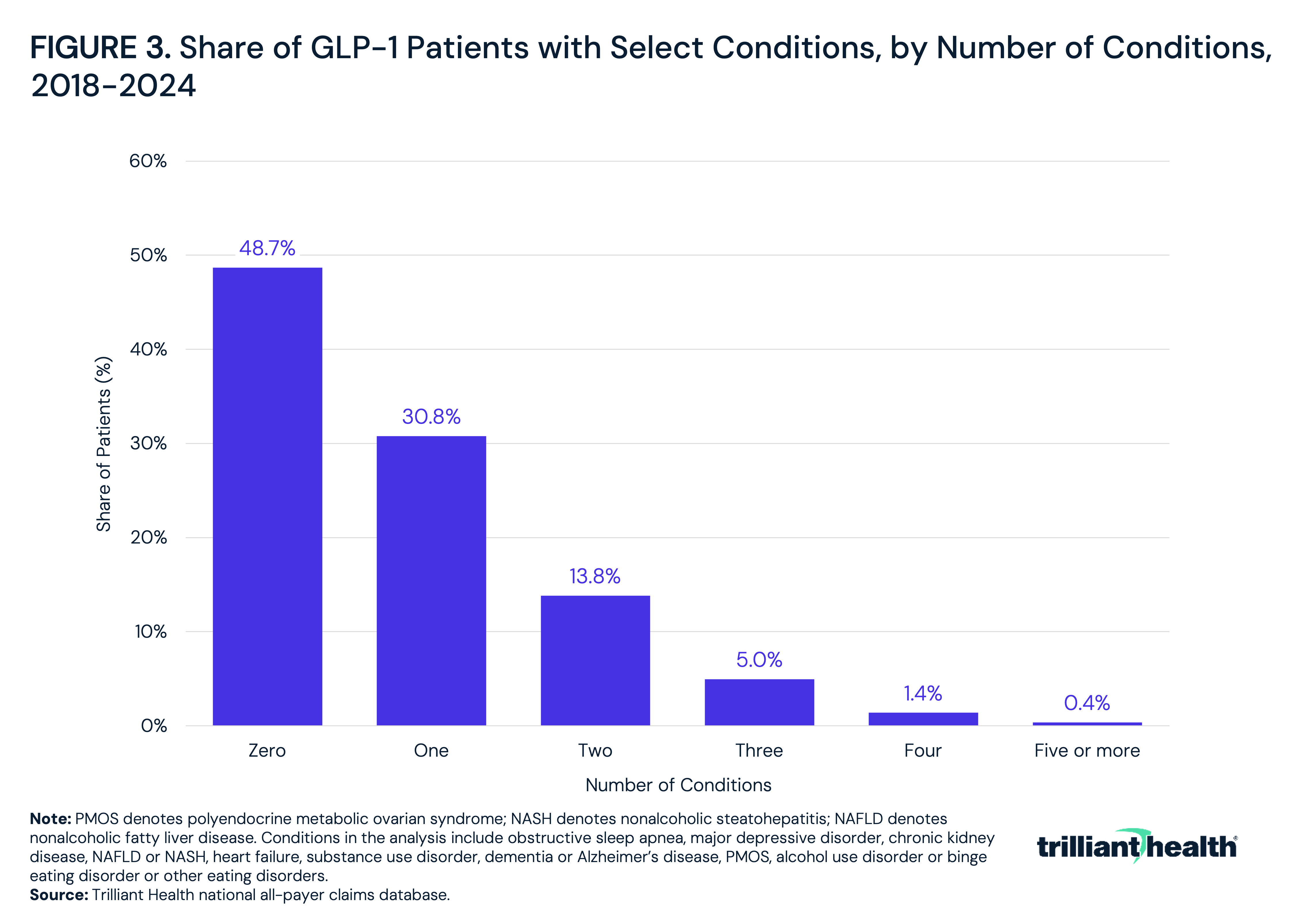
- Slightly more than half of established GLP-1 patients had at least one diagnosis associated with an emerging or recently approved GLP-1 indication.
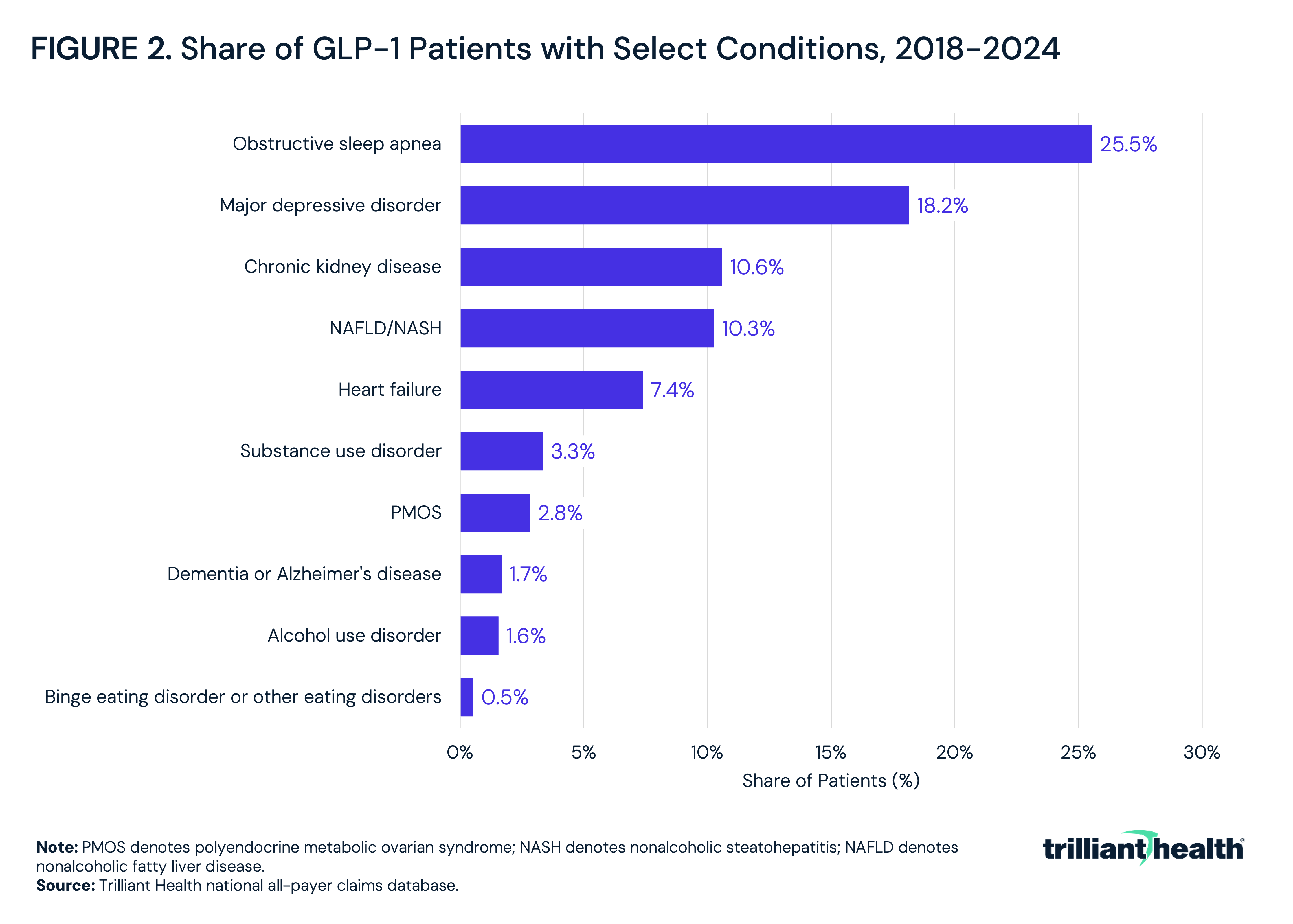
- Obstructive sleep apnea was the most prevalent emerging indication among GLP-1 patients at 25.5%, followed by major depressive disorder at 18.2%.
GLP-1 receptor agonists were initially developed for glycemic control in type 2 diabetes and subsequently approved for chronic weight management. The clinical rationale has broadened, with evidence growing for a range of conditions (i.e., cardiorenal, hepatic, psychiatric, neurologic). While some of these indications have received regulatory approval, others remain in Phase 3 investigation or are prescribed off-label based on earlier-stage evidence. As novel clinical indications are approved, the newly eligible treatment population for each indication inherently would overlap with the population already on GLP-1 therapy. The extent of that overlap, and how it has changed as the GLP-1 prescribing population has grown, has direct implications for coverage policy and utilization management.
Background
The scientific foundation for GLP-1 receptor agonists dates back to the early twentieth century, when researchers first hypothesized that the duodenal mucosa secretes a hormone acting on the pancreas to stimulate insulin release after meals, an effect later named the "incretin effect" by Jean La Barre in 1932.1 GLP-1 was identified in 1986, when researchers found that intestinal L-cells process the proglucagon gene into a truncated peptide that stimulated insulin secretion and suppressed glucagon even in patients with type 2 diabetes, while also reducing appetite.2
In 1992, John Eng at the Veterans Affairs Medical Center identified exendin-4, a peptide that mimicked GLP-1 activity.3 A synthetic derivative, exenatide, was developed in partnership with Eli Lilly as the first GLP-1 receptor agonist approved for type 2 diabetes, which received U.S. Food and Drug Administration (FDA) approval in 2005 as Byetta®.4 Liraglutide (i.e., Victoza®) followed in 2010, dulaglutide (i.e., Trulicity®) in 2014 and semaglutide (i.e., Ozempic®) in 2017. Clinical trials in the 2010s expanded cardiovascular applications within this drug class, with the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial and the Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes (SUSTAIN-6) demonstrating that liraglutide and semaglutide reduced major adverse cardiovascular events (MACE) in type 2 diabetes patients with high cardiovascular risk.5,6 Obesity indications followed next: liraglutide (Saxenda®) in 2014, semaglutide (Wegovy®) in 2021 and tirzepatide (Zepbound®) in 2023.
In December 2024, the FDA approved tirzepatide (Zepbound®) for moderate-to-severe obstructive sleep apnea in adults with obesity, the first pharmacologic approval for that indication.7 In January 2025, semaglutide received FDA approval for chronic kidney disease (CKD) in adults with type 2 diabetes, based on the Evaluate Renal Function with Semaglutide Once Weekly (FLOW) trial, which was the first major trial assessing a GLP-1 receptor agonist's potential to slow CKD progression, stopped early for efficacy after demonstrating a 24% reduction in the primary kidney disease progression endpoint versus placebo.8 The 2024 Kidney Disease: Improving Global Outcomes guidelines and American Diabetes Association standards of care were updated to reflect these findings, listing GLP-1 receptor agonists as recommended agents to reduce cardiorenal risk in patients with CKD and type 2 diabetes.9,10 For non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH), a Phase 2 trial of semaglutide found histological resolution of NASH in 59% of patients versus 17% in the placebo group at 72 weeks.11 In August 2025, semaglutide received accelerated FDA approval for metabolic dysfunction-associated steatohepatitis (MASH) with moderate-to-advanced fibrosis, based on interim Phase 3 trial results in which 62.9% of semaglutide-treated patients achieved steatohepatitis resolution without worsening fibrosis versus 34.3% on placebo.12
Heart failure with preserved ejection fraction represents the most advanced indication currently without a labeled approval. Two Phase 3 trials demonstrated improvements in quality of life, exercise capacity and myocardial stress biomarkers with semaglutide in patients with heart failure and obesity.13 Novo Nordisk resubmitted Wegovy® for a heart failure with preserved ejection fraction indication in early 2025 with an FDA decision originally anticipated in the second half of 2025, subsequently delayed into 2026.
There are early-stage indications where trial evidence is pending or limited. For polyendocrine metabolic ovarian syndrome (PMOS), characterized by insulin resistance and metabolic dysfunction, a 2024 meta-analysis found that GLP-1 receptor agonists reduce BMI, triglycerides, waist circumference and total testosterone in affected women, and international PMOS guidelines recognize them as candidate therapy for overweight and obese patients, but there are not ongoing Phase 3 trials.14,15 For alcohol and substance use disorders, preclinical studies have demonstrated that GLP-1 receptor activation modulates dopamine release in mesolimbic reward circuits, and a pooled meta-analysis found an association with a 36% reduction in alcohol-related events, though trials are ongoing.16 For major depressive disorder, GLP-1 receptors are expressed in brain regions associated with mood regulation, and observational data have generated mixed findings, including both modest antidepressant effects and increased depressive risk in some cohorts.17 A 2025 systematic review found significant improvements in Binge Eating Scale scores with GLP-1 receptor agonist use, though evidence remains limited to small-scale trials.18 For Alzheimer's disease and dementia, a Phase 2b trial of liraglutide generated encouraging early signals, but Phase 3 trials of semaglutide, enrolling approximately 1,800 patients with early Alzheimer's disease, did not demonstrate clinical benefit when results were reported in late 2025.19,20,21
This analysis examines the degree to which patients already receiving GLP-1 therapy also have one or more diagnoses associated with conditions where the drug class has demonstrated or hypothesized clinical benefit.
Analytic Approach
National all-payer claims data were leveraged to analyze a GLP-1 patient cohort between 2018 and 2024. Analyzed patients were required to have at least two filled pharmacy claims for any GLP-1 receptor agonist in two distinct years and be ages 18 and older, regardless of the indication for which the GLP-1 was prescribed.
Ten emerging indication categories were evaluated based on the presence of at least one relevant ICD-10-CM diagnosis code at any point during the study period: PMOS, obstructive sleep apnea, NAFLD or NASH, CKD, heart failure, alcohol use disorder, substance use disorder, major depressive disorder, binge eating disorder or other eating disorders and Alzheimer's disease or dementia. Patient volume over time, along with the share of the GLP-1 patient cohort with at least one of these conditions, was analyzed.
Findings
GLP-1 patient volume increased by 635.6% from 2018 to 2024 (Figure 1). The pattern of growth aligns with the 2021 Wegovy® approval and subsequent obesity indication expansion.
Across the ten emerging indications examined, obstructive sleep apnea was the most common co-occurring diagnosis, present in 25.5% of GLP-1 patients between 2018 and 2024, followed by major depressive disorder at 18.2%, CKD at 10.6% and NAFLD/NASH at 10.3% (Figure 2). Binge eating disorder or other eating disorders was least common at 0.5%.
Among GLP-1 patients between 2018 and 2024, 48.7% had none of the ten emerging indication diagnoses examined. Nearly one-third had one condition (30.8%), 13.8% had two, 5.0% had three, 1.4% had four and 0.4% had five or more (Figure 3).
Conclusion
More than half of GLP-1 patients had at least one diagnosis associated with a condition for which GLP-1 therapy is approved, recently approved, under active clinical investigation or hypothesized by clinicians and researchers. The conditions with the highest co-occurrence are obstructive sleep apnea at 25.5% and major depressive disorder at 18.2%. Given that many of these conditions (e.g., obstructive sleep apnea, major depressive disorder, heart failure) are highly prevalent in the metabolically complex populations most likely to be prescribed GLP-1 therapy, a substantial share of patients may already be deriving clinical benefit from the drug across multiple conditions simultaneously, whether or not those benefits are recognized or documented at the point of prescribing.
For payers and pharmacy benefit managers (PBMs), the data have direct implications for coverage policy design. As the FDA-approved indication list expands, the share of GLP-1 patients with a clinically defensible basis for drug coverage will grow. If the majority of adults in a risk pool are prescribed GLP-1 therapy – across a combination of approved, off-label and investigational indications – at list prices that have remained high despite incremental reductions, the aggregate cost exposure will become difficult to manage through traditional utilization controls. For self-funded employers, the question is no longer whether GLP-1 coverage is appropriate for a given indication, but whether the healthcare system can sustain broad coverage of a high-cost chronic therapy across an increasingly large and diagnostically heterogeneous population.
The conditions examined here are broadly prevalent in the U.S. adult population. An estimated 83.7M U.S. adults – approximately 32.4% of the adult population – had obstructive sleep apnea in 2024.22 An estimated 21M adults had at least one major depressive episode in 2021, representing 8.3% of the U.S. adult population.23 An estimated 37M adults, or one in ten, have CKD.24 As GLP-1 adoption continues to broaden across approved indications, off-label emerging indications and discretionary off-label prescribing for weight loss in patients without a qualifying comorbidity, the pool of adults with both a GLP-1 prescription and a diagnosis associated with an emerging indication will expand. The more consequential economic question is what happens if list prices remain high as that population grows. GLP-1 therapies are chronic treatments with clinical benefit contingent on sustained use, and discontinuation is associated with reversal of effect. A healthcare system in which a large and growing share of adults are indefinitely on a drug with a monthly cost of several hundred dollars, across a widening range of indications with variable evidentiary support, faces a spending trajectory that utilization management alone is unlikely to contain. The policy and economic case for accelerating price competition, generic entry and biosimilar development is directly proportional to how broadly these drugs are ultimately prescribed.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
