























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
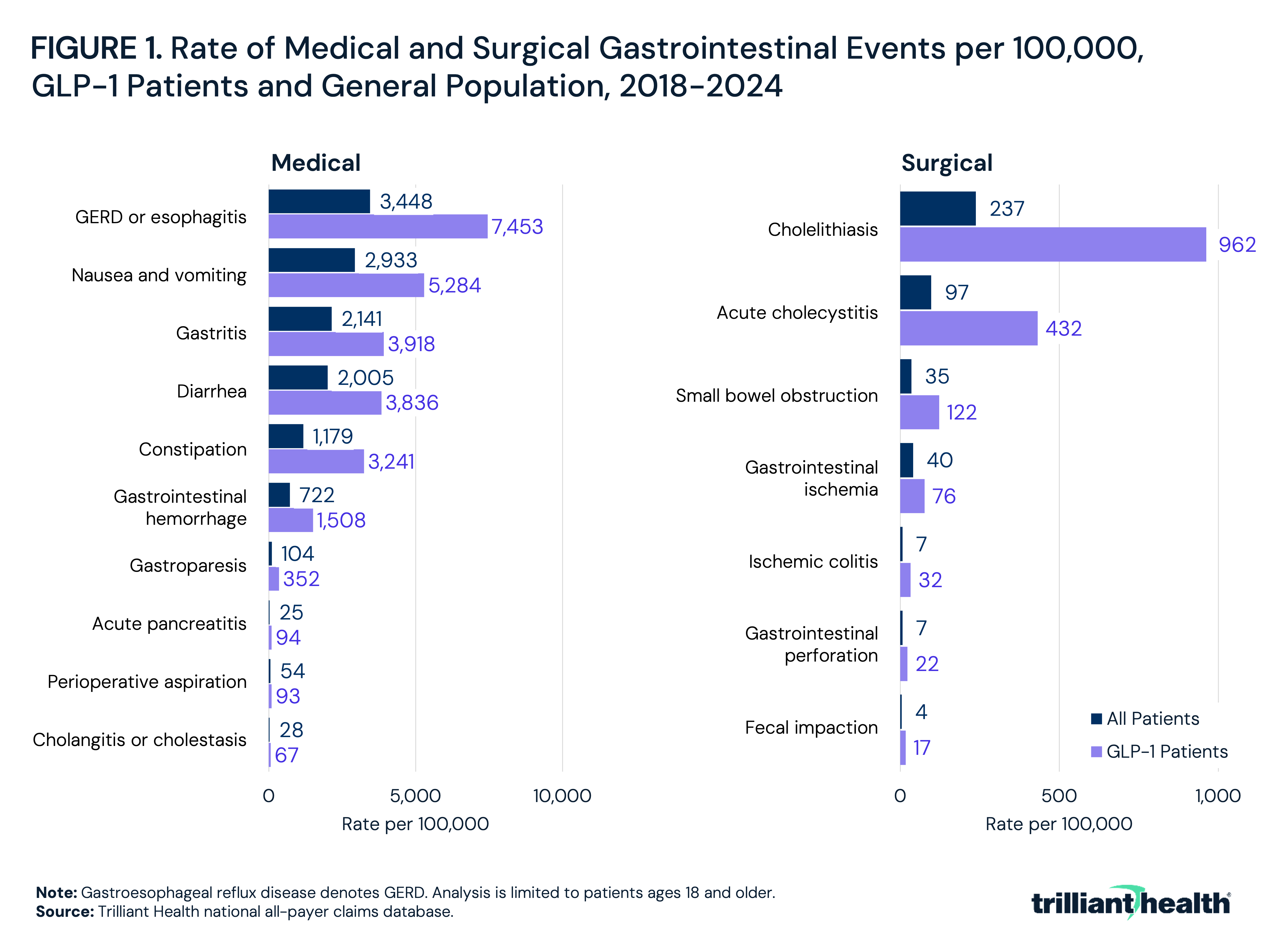
- GLP-1 patients without preexisting GI motility disorders had GERD or esophagitis at a rate of 7,453 per 100,000, compared to 3,448 per 100,000 among the general population.
- Cholelithiasis was the most common surgical GI event among GLP-1 patients, occurring at a rate of 962 per 100,000 compared to 237 per 100,000 in the general population, consistent with FDA labeling that documents biliary disease risk for semaglutide.
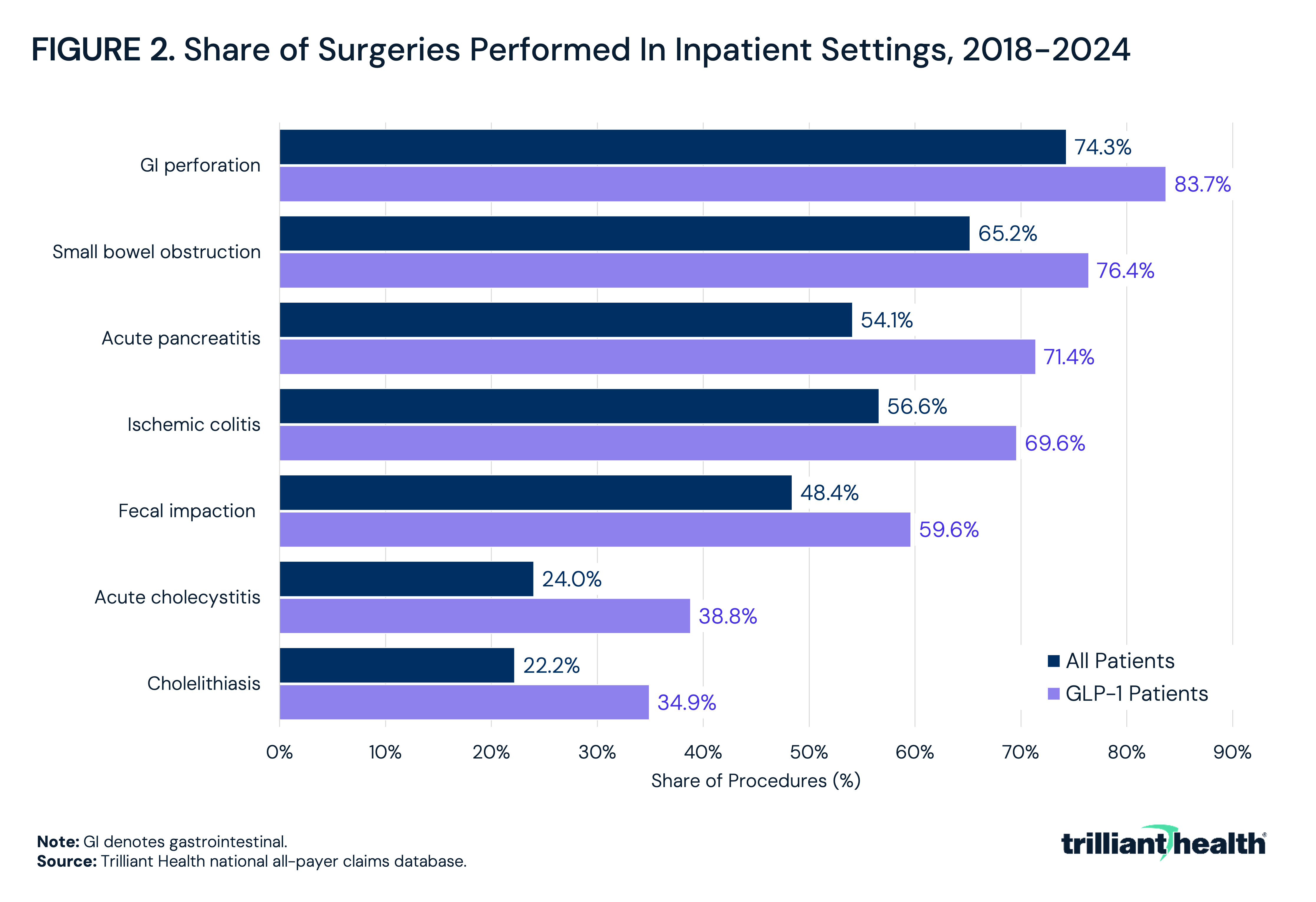
- Across all seven GI surgical events examined, GLP-1 patients were managed inpatient at higher rates than the general population, with the largest absolute gap observed for acute pancreatitis, where 71.4% of GLP-1 patients had inpatient surgery compared to 54.1% of all patients.
GLP-1 receptor agonists are among the fastest-growing drug classes in the U.S., with patient volume increasing by 635.6% from 2018 to 2024.1 Accompanying that growth is an expanding body of evidence on adverse gastrointestinal (GI) effects, ranging from nausea and vomiting to complications requiring surgical intervention. Notably, the GI side effects of GLP-1s, some of which the U.S. Food and Drug Administration (FDA) first mandated disclosure in 2005 and expanded in 2007, are a direct consequence of the same receptor activity that drives therapeutic benefit.2,3
The evidence on serious GI side effects and risks associated with GLP-1s is mixed. Randomized controlled trial (RCT) meta-analyses have not broadly confirmed statistically significant increases in surgical GI events, except for cholelithiasis and biliary disease, which has been reflected in FDA drug labeling for semaglutide. However, observational data have produced stronger signals, including elevated small bowel obstruction risk. As the number of patients using a GLP-1 continues to expand, potential downstream side effects and surgical risk can translate to meaningful clinical and economic exposure.
Background
GLP-1 receptors are expressed throughout the GI tract (i.e., stomach, small intestine, colon and gallbladder) where agonist activity slows gastric emptying, reduces intestinal peristalsis and disrupts the migrating motor complex, the cyclical motility pattern responsible for clearing the stomach and small bowel between meals. The biliary system is most susceptible to potential adverse events, given rapid weight loss accelerates cholesterol saturation of bile, and GLP-1-mediated gallbladder stasis reduces bile flow, creating conditions that lead to gallstone formation.4 Cholelithiasis has been confirmed as a statistically significant risk across 55 RCTs reflecting more than 106,000 participants, and FDA labeling for semaglutide includes warnings for acute gallbladder disease, including cholecystitis.5,6
Current evidence indicating small bowel obstruction is less conclusive. Observational studies, including pharmacovigilance analyses and retrospective cohort studies, report elevated obstruction risk in GLP-1 patients, particularly among those with prior abdominal surgery or adhesions.7,8,9 The European Medicines Agency flagged cases of intestinal obstruction linked to delayed gastric emptying reflective of gastroparesis as early as 2013.10 While the meta-analysis of 55 RCTs did not find a statistically significant increase in GI perforation or bowel obstruction, the authors noted that trial populations may underrepresent patients with the highest baseline risk for GI obstruction. Notably, in 2023, the American Society of Anesthesiologists issued guidance regarding perioperative risk and recommended that daily-dose GLP-1 receptor agonists be withheld on the day of a procedure and weekly-dosed formulations be withheld for one week prior, given the documented risk of residual gastric content and pulmonary aspiration under sedation.11
This analysis uses national all-payer claims data to characterize the rate of medical and surgical GI events among established GLP-1 patients without preexisting GI motility disorders.
Analytic Approach
National all-payer claims data were used to construct an established GLP-1 patient cohort from 2018 through 2024. Patients were required to have at least two filled pharmacy claims for any GLP-1/gastric inhibitory polypeptide (GIP) receptor agonist across two distinct calendar years and to be age 18 or older at the time of the first filled claim. To isolate the GI risk attributable to GLP-1 exposure rather than preexisting disease, patients with any of the following conditions documented prior to their first GLP-1 claim were excluded: gastroparesis, gastric motility disorders, Crohn's disease or inflammatory bowel disease, prior bowel obstruction, intestinal adhesions, chronic constipation or irritable bowel syndrome, gallstone disease and chronic pancreatitis.
Medical and surgical GI events were identified using ICD-10-CM diagnosis codes and, for surgical events, relevant procedure codes. Surgical events included cholelithiasis, acute cholecystitis, small bowel obstruction, GI ischemia, acute pancreatitis, GI perforation, fecal impaction and ischemic colitis. Medical events included GERD (gastroesophageal reflux disease) or esophagitis, nausea and vomiting, gastritis, diarrhea, constipation, GI hemorrhage, gastroparesis, acute pancreatitis, perioperative aspiration and cholangitis or cholestasis. Incidence was expressed as a rate per 100,000 patients and compared between the GLP-1 cohort and a general patient population benchmark. For surgical events, the share of procedures performed in an inpatient vs. outpatient setting was calculated for both GLP-1 patients and the general patient population.
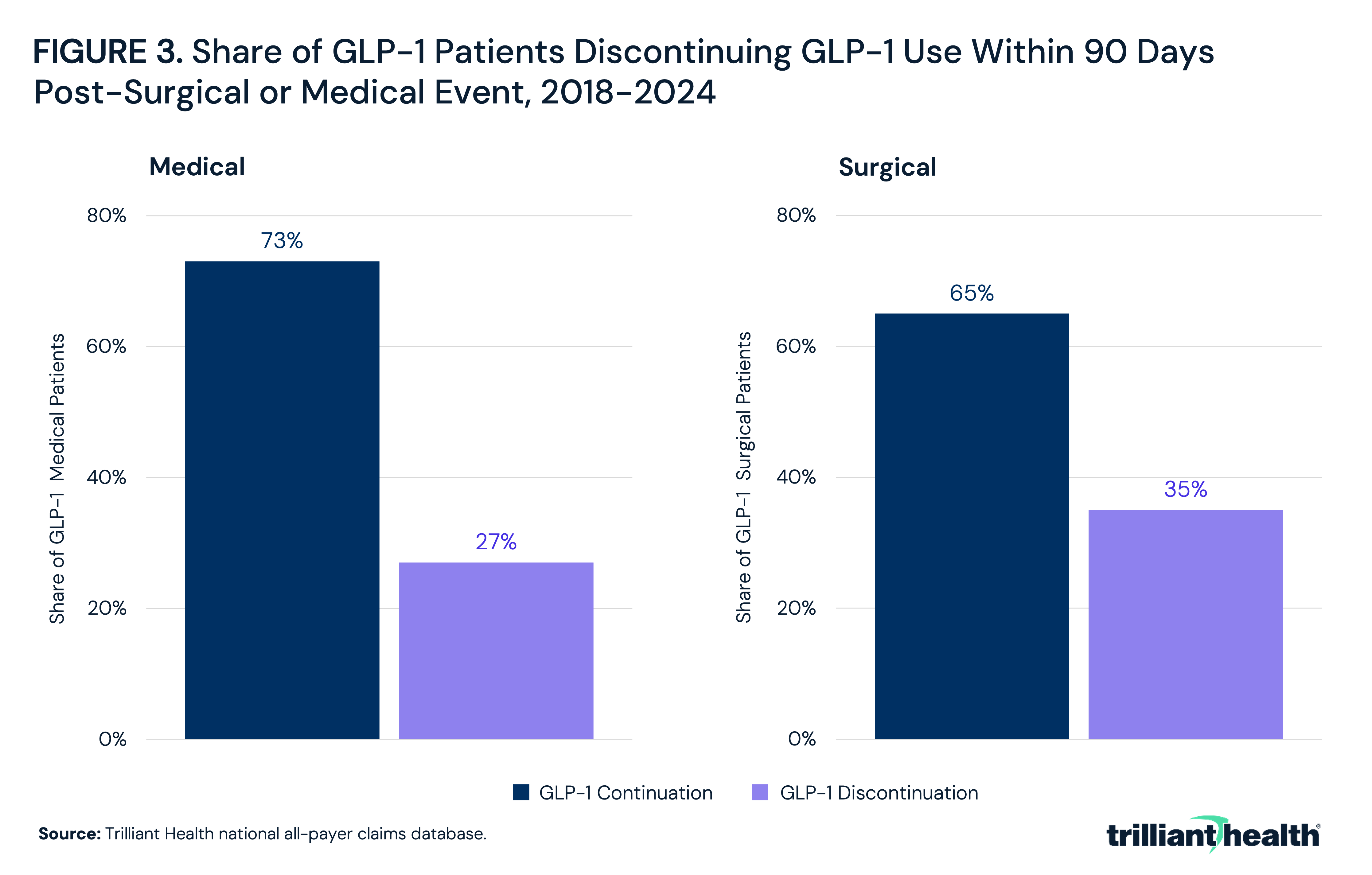
GLP-1 therapy continuation following a surgical or medical GI event was assessed among GLP-1 patients who experienced at least one surgical or medical GI event. Continuation was defined as at least one GLP-1 pharmacy fill within 90 days of the surgical event date. Discontinuation was defined as no GLP-1 claim within 90 days following the event.
Findings
Across all medical GI events examined, rates were higher in the GLP-1 cohort than in the general patient population (Figure 1). GERD or esophagitis was the most prevalent medical GI event, with a rate of 7,453 per 100,000 GLP-1 patients compared to 3,448 per 100,000 in the general population. The rate of nausea and vomiting was 5,284 per 100,000 GLP-1 patients and 2,933 in the general population. Gastroparesis had a rate of 352 per 100,000 GLP-1 patients compared to 104 per 100,000 in the general population. The rate of acute pancreatitis was 94 per 100,000 GLP-1 patients and 25 per 100,000 in the general population.
Among surgical GI events, cholelithiasis was the most common, with a rate of 962 per 100,000 GLP-1 patients compared to 237 per 100,000 in the general population. The rate of acute cholecystitis was 432 per 100,000 GLP-1 patients and 97 per 100,000 in the general population. The rate of small bowel obstruction was 122 per 100,000 GLP-1 patients compared to 35 per 100,000 in the general population. The ischemic colitis rate was 32 per 100,000 GLP-1 patients and seven per 100,000 in the general population.
GLP-1 patients undergoing GI surgery were more likely to be treated in higher cost inpatient settings than the general patient population across all seven conditions. GI perforation had the highest inpatient share among GLP-1 patients at 83.7%, compared to 74.3% in the general population (Figure 2). Small bowel obstruction had the second highest inpatient share, with 76.4% of GLP-1 patients compared to 65.2% of all patients. The largest absolute gap between GLP-1 patients and the general population was observed for acute pancreatitis, where 71.4% of GLP-1 patients had inpatient surgery compared to 54.1% of all patients. Ischemic colitis had inpatient rates of 69.6% among GLP-1 patients and 56.6% among all patients. Even for conditions more commonly managed in outpatient settings, GLP-1 patients had higher inpatient shares: fecal impaction at 59.6% compared to 48.4% of all patients, acute cholecystitis at 38.8% compared to 24.0% and cholelithiasis at 34.9% compared to 22.2%.
Among GLP-1 patients who had a surgical GI event, 65% had at least one GLP-1 pharmacy fill within 90 days of the surgical event, indicating continued use of the drug class following surgery (Figure 3). The remaining 35% did not have a GLP-1 claim within 90 days following the event, meeting the operational definition of discontinuation. Among GLP-1 patients who had a medical GI event, 73% had at least one GLP-1 pharmacy fill within 90 days of the medical event, and the remaining 27% did not have a GLP-1 claim within 90 days.
Conclusion
The rapid adoption of GLP-1 therapies and increasing utilization for a variety of clinical conditions is arguably the most impactful development in the health economy in the past decade. Whether to include GLP-1 therapies as a covered benefit has been the subject of intense debate for employers and health insurers alike, but almost exclusively with respect to the cost of GLP-1s. The findings suggest that the risks of GLP-1 therapies, which the FDA first identified more than 20 years ago, should be included in the cost/benefit analysis for every employer and health insurer.
Over the 2018 to 2024 study period, GLP-1 patients without preexisting GI motility disorders had substantially higher rates of both medical and surgical GI events than the general patient population. Cholelithiasis and acute cholecystitis accounted for the highest absolute burden among surgical events, consistent with the biological plausibility of GLP-1-mediated gallbladder stasis and FDA-mandated labeling that documents biliary disease risk. Small bowel obstruction and ischemic colitis, while less frequent, also occurred at higher rates in GLP-1 patients, a finding that aligns with observational literature identifying motility disruption as having a risk for GI obstruction.
Across all GI surgeries examined, GLP-1 patients underwent surgeries in higher cost inpatient settings at higher rates than the general patient population. Whether this reflects greater case severity, delayed presentation or patient complexity independent of GI disease cannot be conclusively assessed, but the pattern is consistent across complication types and suggests that when GLP-1 patients experience a surgical GI event, it tends to be a more resource-intensive episode than a comparable surgical event in the general population.
The findings also raise questions about prescribing oversight. Patients initially prescribed GLP-1 therapy through direct-to-consumer (DTC) channels may lack access to the clinical evaluation necessary to identify preexisting GI risk factors or contraindications prior to treatment. Notably, the FDA does not regulate the prescribing act itself, regardless of whether a medication is prescribed in person or through a DTC platform, leaving clinical oversight of DTC prescribing to state medical boards, which may be particularly consequential for patients initiating GLP-1 therapy without an established provider relationship or baseline clinical assessment. Formulary and prior authorization designs that rely primarily on BMI or glycemic thresholds reflect the original approved use case for diabetes and do not screen for GI risk or other risks related to the rapidly expanding number of uses of GLP-1 therapies. The absence of baseline GI history assessment may leave at-risk patients without appropriate monitoring protocols for early symptom recognition or sufficient information to allow informed consent. The surgical complications, such as small bowel obstruction and ischemic colitis, which can present subtly before becoming emergent, underscore the clinical value of targeted screening prior to therapy initiation and ongoing surveillance of GI-related adverse events.
For payers and pharmacy benefit managers (PBMs), these findings have implications for the total cost of care associated with GLP-1 coverage. Notably, Medicare Part D spending was substantially higher in 2025 than past years, with the Medicare Trustees citing GLP-1 utilization as a key spending driver.12 As the GLP-1 prescribing population grows, the absolute number of GLP-1 patients that could experience a downstream GI surgical event will increase proportionally. Whether the increased prescribing for other non-diabetic use cases will result in other unforeseen complications is logically an issue for the FDA’s consideration.
In addition to the increased incidence of medical and surgical events from complications from GLP-1s, the consistent trends in higher inpatient management rates documented here suggest that the costs associated with GI surgical events in this population are meaningfully greater than in the general population. For self-funded employers and health plans managing both drug cost and downstream medical cost, the surgical GI risk profile of GLP-1 patients is a component of total cost modeling that has not been well characterized at scale.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
