























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
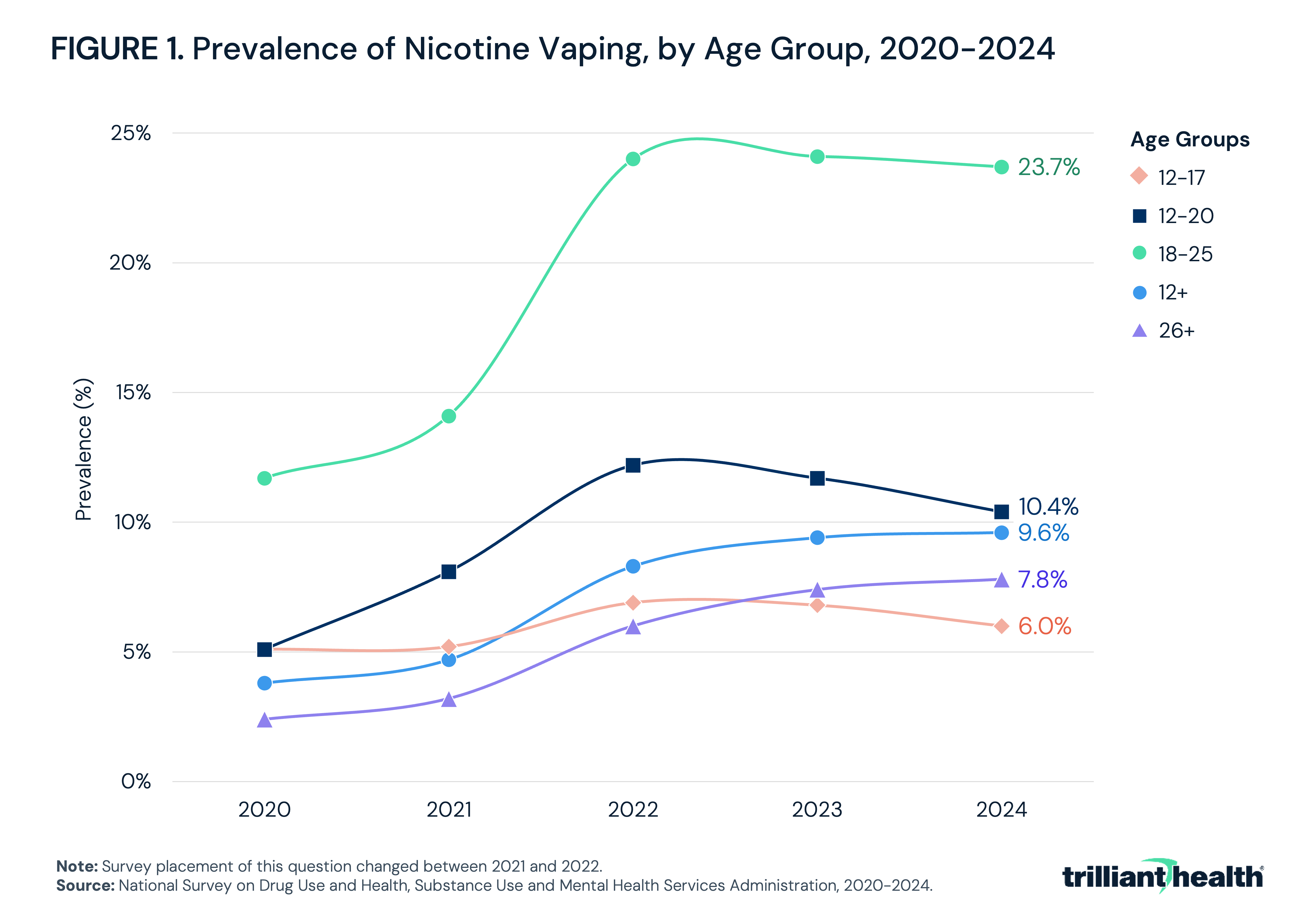
- Nicotine vaping prevalence among adults ages 18-25 more than doubled from 11.7% in 2020 to 23.7% in 2024, with overall prevalence among Americans ages 12 and older increasing nearly 3x.
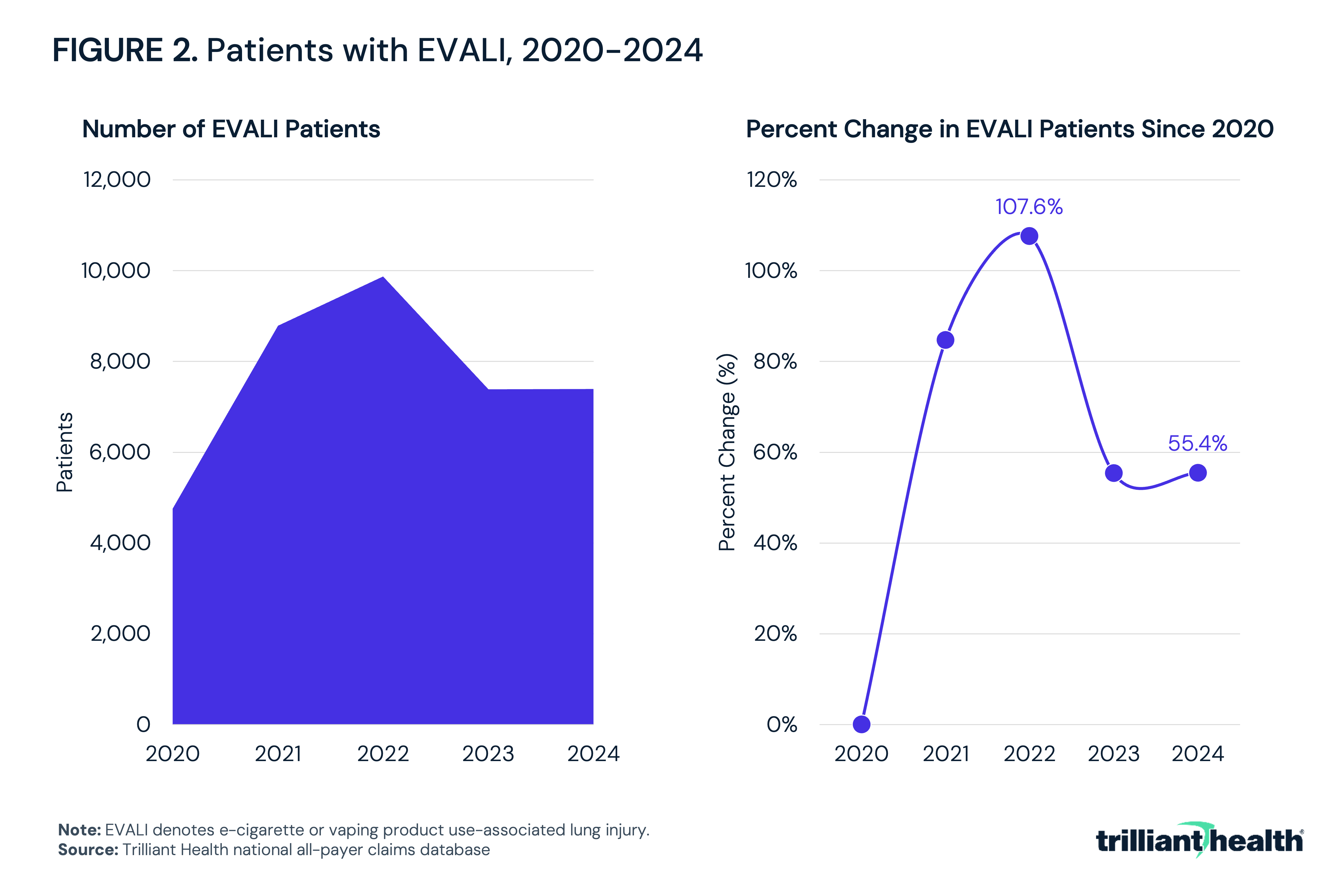
- E-cigarette or vaping product use-associated lung injury patient volume peaked in 2022 at 107.6% above the 2020 baseline before declining to 55.4% above the baseline in 2024.
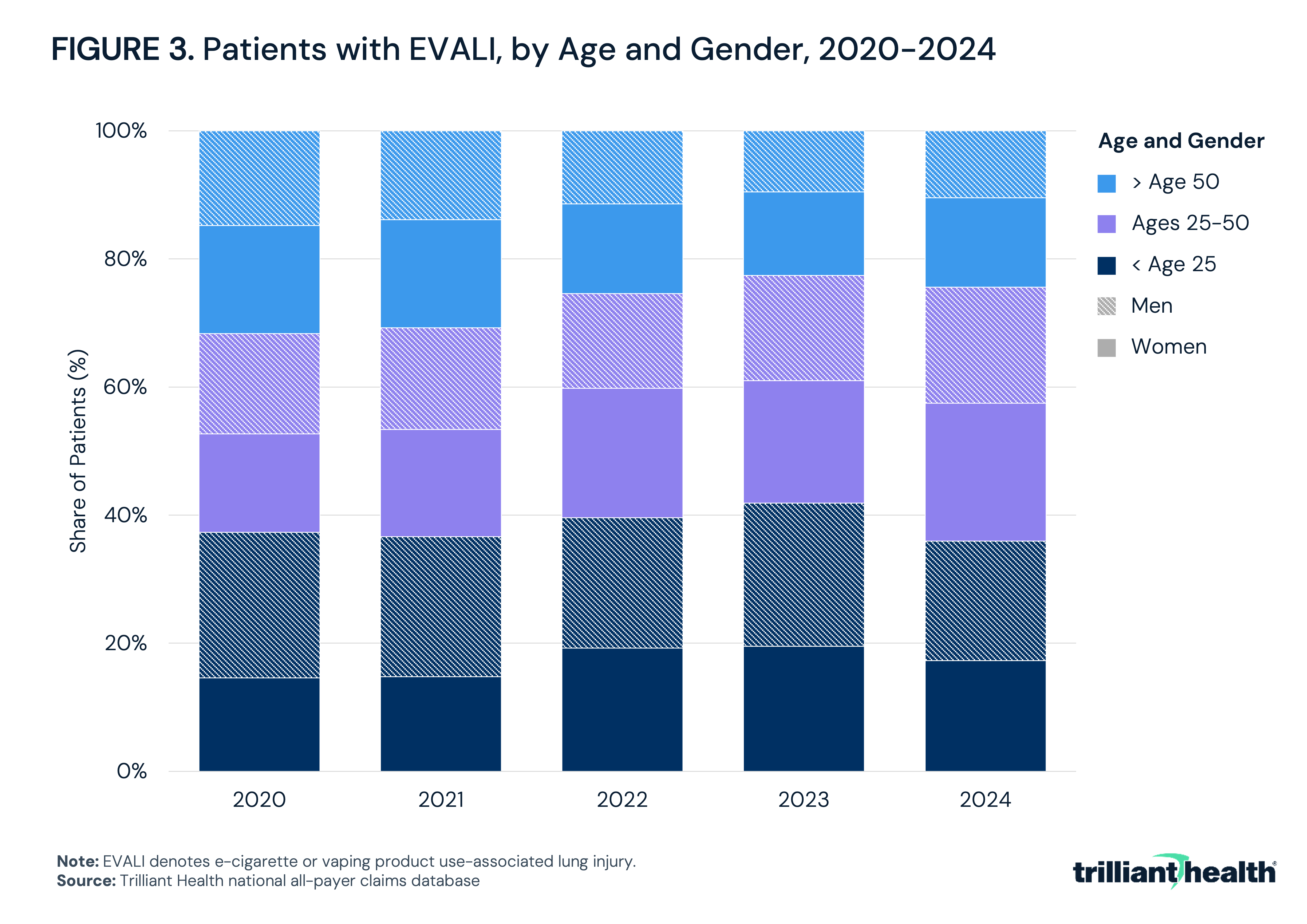
- The share of female EVALI patients increased across the study period, with those ages 25–50 representing the fastest-growing demographic subgroup.
Electronic cigarettes and vaping products have expanded rapidly in the U.S., transitioning from smoking cessation tools to broadly adopted consumer products, particularly among adolescents and young adults. Awareness of the acute clinical harms associated with vaping has grown alongside expanded use. E-cigarette or vaping product use-associated lung injury (EVALI) is the most severe and well-documented medical condition stemming from vaping.1,2 EVALI is an acute or subacute respiratory illness affecting primarily young, otherwise healthy individuals, often requiring intensive hospital-based care. The surge of EVALI cases in 2019 drew public and regulatory focus. However, the broader pattern of vaping-related injury remains incompletely characterized at the population level, in part because consistent clinical recognition and documentation of EVALI has not been broadly achieved.
Background
E-cigarette use has grown substantially in the U.S. in the last 15 years, driven by the products' initial positioning as a lower-risk alternative to combustible cigarettes and, increasingly, by marketing targeted to younger consumers. The Substance Abuse and Mental Health Services Administration (SAMHSA) survey data show nicotine vaping among people ages 12 and older increased more than 2.5x from 3.8% in 2020 to 9.6% in 2024 (Figure 1).3,4 Prevalence was highest among young adults ages 18-25, increasing from 11.7% to 23.7% in the same time period. The same surveys found overall vaping prevalence among adolescents ages 12-20 doubled from 5.1% to 10.4% between 2020 and 2024. Notably, by 2017, researchers reported that e-cigarettes had become the most common first tobacco product used by adolescents.5 Other surveillance data suggests that youths who vape nicotine may be hardening into a more nicotine-dependent, treatment-resistant population over time, as evidenced by shifts toward daily vaping and difficulty quitting.6 Unlike older adults managing established tobacco dependence, younger users are often initiating vaping without a prior smoking history.
EVALI became a recognized clinical diagnosis in the summer of 2019, when the Centers for Disease Control and Prevention (CDC) began investigating an uptick in hospitalizations among patients reporting recent vaping product use. Cases peaked in September 2019 and, by February 2020, more than 2,800 hospitalizations and 68 deaths had been reported to the CDC across all 50 states and two U.S. territories.7 The affected population skewed young and male – with a median non-fatal patient age of 24 – and the majority reported using THC-containing products.8 Patients with fatal cases were substantially older than those who survived, with a median age of 51 compared to 24, and were more likely to have preexisting cardiac disease, obesity, respiratory illness or mental health condition. These patterns point to a condition whose severity is shaped not only by the exposure itself but by underlying comorbidities and overall health status. Following public health intervention and the removal of vitamin E acetate – a diluent identified in lung fluid samples from the overwhelming majority of EVALI patients – from many products, reported case counts declined sharply. However, EVALI cases have persisted, and researchers have emphasized that other unidentified compounds in both THC- and nicotine-containing products may contribute to lung injury in ways not yet fully understood.9
Part of what makes EVALI difficult to study at scale is that it is a diagnosis of exclusion. CDC diagnostic criteria require a history of vaping product use in the 90 days preceding symptom onset, pulmonary infiltrates on imaging and the absence of other plausible diagnoses (e.g., pneumonia, influenza or COVID-19).10 Patients may be reluctant to disclose vaping product use, particularly when THC is involved, and clinicians rarely screen for it.
Despite these challenges, the prevalence of vaping and the associated public health concern support an examination of trends in EVALI and other vaping-related respiratory encounters, particularly in light of recent guidance from the U.S. Food and Drug Administration (FDA).11
Analytic Approach
National all-payer claims data were leveraged to analyze patient volume for EVALI from 2020-2024 using the ICD-10-CM code U07.0, which was formalized in April 2020. Patients were also analyzed by age and gender.
Findings
Following the April 2020 formalization of U07.0, EVALI patient volume increased 84.7% from 2020 to 2021 and peaked in 2022 at 107.6% above the 2020 baseline (Figure 2). Volume declined to 55.4% above baseline in 2023 and remained at that level through 2024.
The demographic composition of EVALI encounters shifted meaningfully between 2020 and 2024. Men represented 53.2% of EVALI patients in 2020, with men under 25 accounting for 22.8% alone (Figure 3). By 2024, men represented 47.3% of patients, with women representing a slight majority for the first time in the study period. Notably, women ages 25-50 increased in share from 15.4% in 2020 to 21.5% in 2024. Concurrently, both men and women over age 50 represented a declining share of patients, with men falling from 14.8% to 10.5% and women from 16.9% to 14.0%.
Conclusion
The public health response to the 2019 EVALI outbreak revealed the degree to which the clinical and surveillance infrastructure for vaping-related harm was built reactively rather than proactively. EVALI patient volume more than doubled from 2020 to its 2022 peak before moderating yet remained more than 55% above the 2020 baseline through 2024. The initial rise likely reflects a combination of incident cases and growing clinician adoption of U07.0 following its introduction, though this period coincides with the COVID-19 pandemic – which likely both complicated EVALI recognition given significant symptom overlap between the two conditions, and altered broader healthcare utilization patterns in ways that may have influenced encounter volume in either direction. The persistence of elevated volume through 2023 and 2024, as pandemic-related disruptions subsided and vaping prevalence among young adults continued to grow, suggests ongoing clinical burden rather than resolution of the underlying problem.
Underdiagnosis driven by patient non-disclosure, symptom overlap with common respiratory infections – including COVID-19 – and inconsistent application of U07.0 mean that encounter volume likely understates the true burden. This is particularly relevant given evidence that the youth and young adult vaping population is becoming more chronic over time. As overall adolescent prevalence declines, those who continue to vape are doing so more heavily and with increasing difficulty quitting, while prevalence among young adults continues to grow. The shifting demographic profile of EVALI patients observed in this analysis, particularly the growing share of women and adults ages 25-50, is consistent with these broader population trends and may signal continued evolution in the clinical presentation of vaping-related lung injury.
Regulation of e-cigarettes has evolved considerably since the 2019 outbreak, though gaps remain. The FDA has broad authority to regulate e-cigarette products under the Tobacco Control Act, and several states have enacted their own restrictions on flavored products and online sales. Nevertheless, the e-cigarette market continues to outpace regulatory response more broadly. New product formats, novel chemical formulations and disposable devices have proliferated, creating ongoing exposure pathways that differ meaningfully from those implicated in the original EVALI cases.
On May 5, 2026, the FDA authorized four flavored electronic nicotine delivery system (ENDS) products from Glas – the first authorization of non-tobacco, non-menthol flavored ENDS – bringing the total number of lawfully authorized ENDS products to 45, a fraction of what remains on the market illegally.12 This authorization comes as EVALI encounter volume remains elevated, the youth vaping population is hardening and the long-term pulmonary consequences of sustained vaping exposure are still being fully understood.
The stated rationale for the ENDS authorization hinged on device-level age verification technology designed to mitigate youth access, reflecting a regulatory posture increasingly oriented toward adult consumer access, rather than the elimination of nicotine product risk. Whether device-based age-gating proves effective at limiting youth exposure in practice remains to be seen. Regulatory decisions made based on relative risk today will shape the clinical burden that clinicians and health systems manage for years to come.
For decades, declining smoking rates represented one of public health's clearest successes, resulting from regulatory interventions, litigation, cultural shifts, public health campaigns and clinical intervention. E-cigarettes have disrupted that trajectory, introducing a new generation to nicotine dependence, often under the guise of harm reduction. The influx of EVALI cases in 2019 made those consequences clear. The clinical burden documented here through a relatively small but persistent volume of EVALI patient encounters and a growing at-risk youth population is a reminder that the work of protecting population health from nicotine-related harm is still active and ongoing.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
