























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
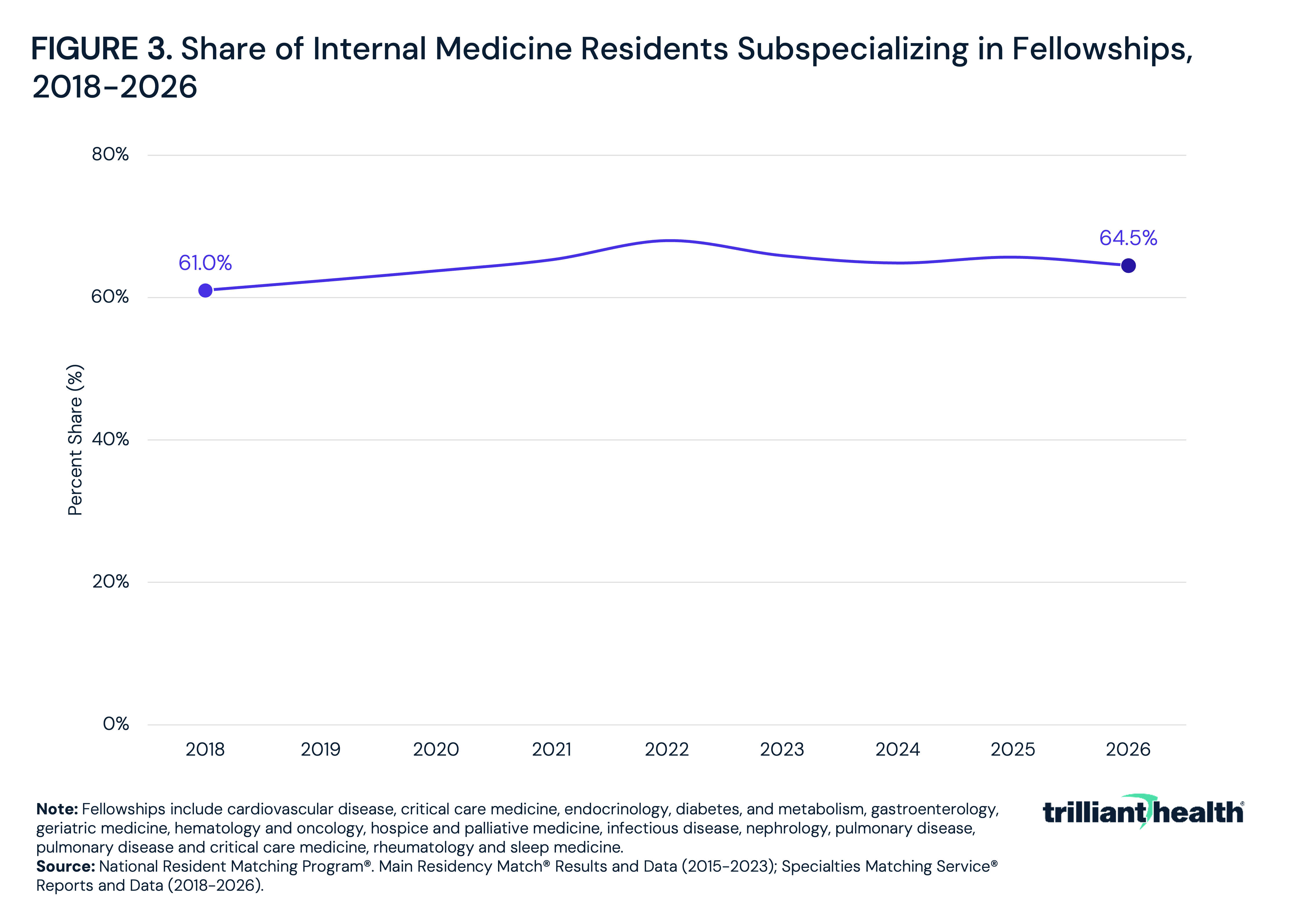
- Internal medicine residents continue to pursue subspecialty fellowships at increasing rates, rising from 61.0% in 2018 to 64.5% in 2025, with a peak of 68.0% in 2022.
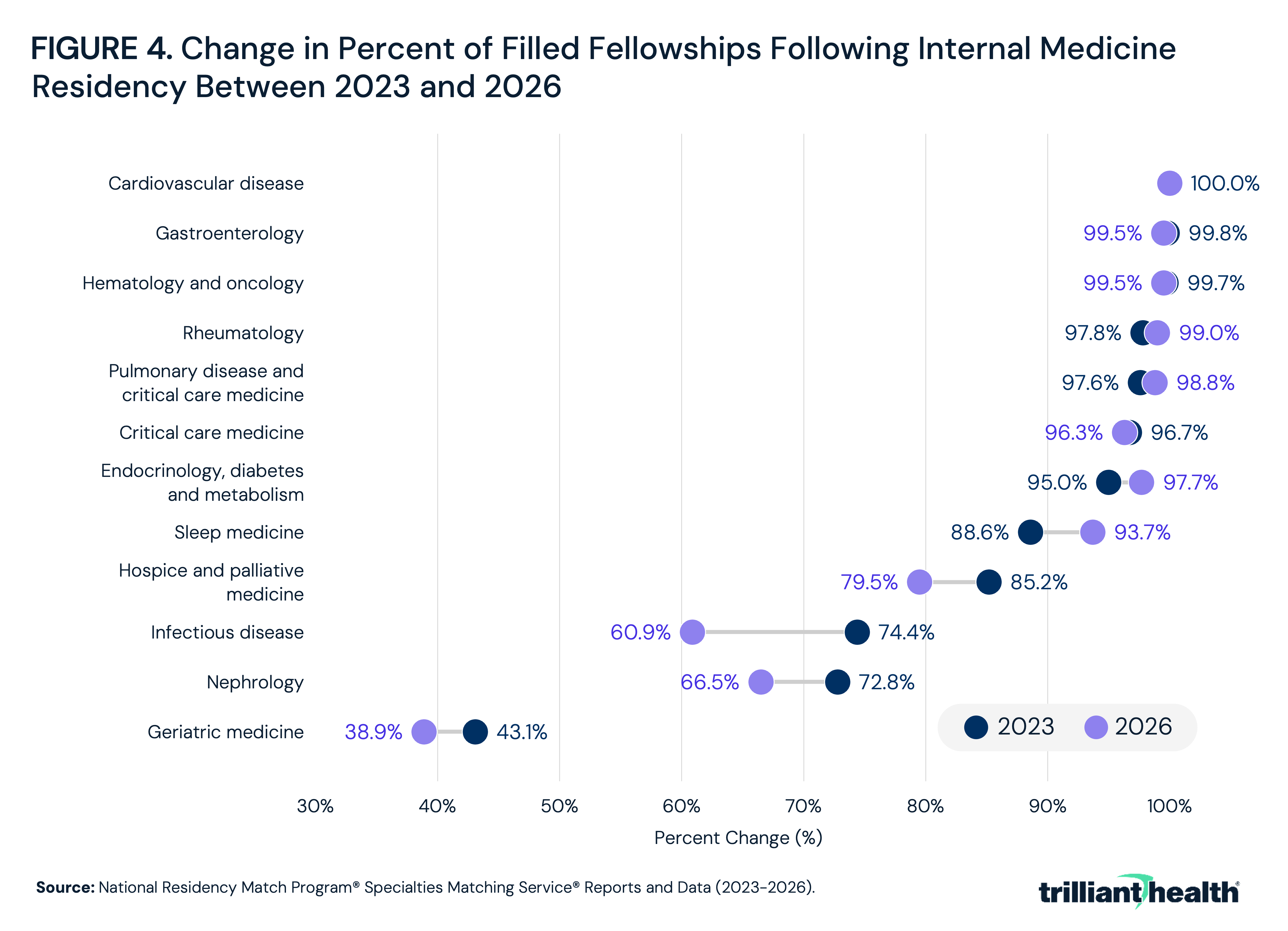
- Cardiovascular disease (100.0%), hematology and oncology (99.5%) and gastroenterology (99.5%) had the highest fellowship fill rates in 2026, remaining among the most competitive internal medicine subspecialties.
- Since 2023, fellowship fill rates have declined sharply in low-supply fields directly relevant to an aging U.S. population. Between 2023 and 2026, geriatric medicine fell from 58.7% to 38.9%, infectious disease from 80.4% to 60.9% and hospice and palliative medicine from 97.2% to 79.5%.
- Fellowship fill rates in 2026 varied substantially by state, with geriatric medicine ranging from 16.7% in Virginia to 76.5% in Massachusetts and more than a dozen states not offering geriatric medicine fellowship positions.
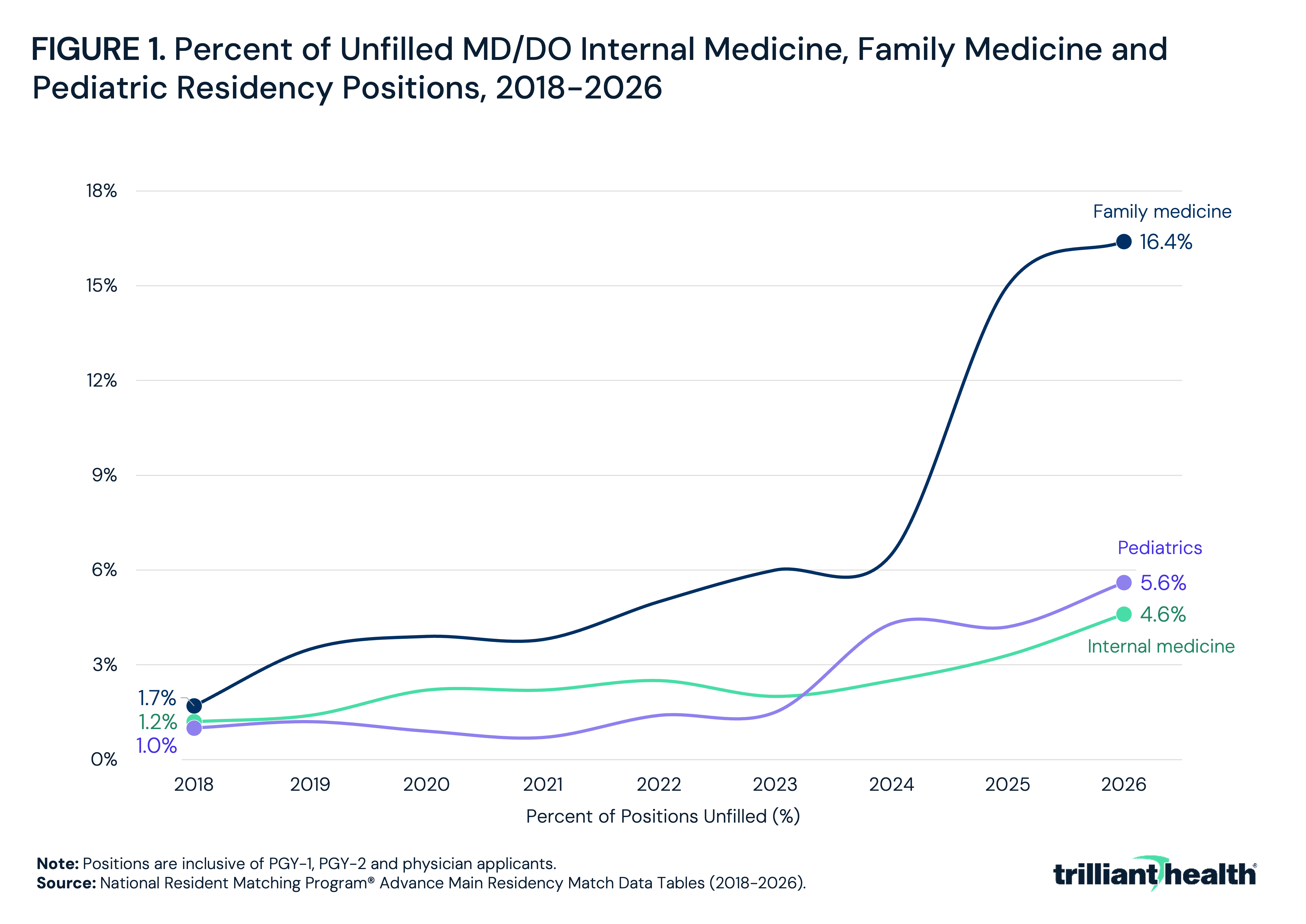
The 2026 Residency Match Results and Data, analyzed earlier this year, revealed that primary care residencies (i.e., family medicine, pediatrics and internal medicine) once again had among the highest vacancy rates at 16.4%, 5.6% and 4.6%, respectively (Figure 1).1 With the July 1 start date for most residencies and fellowships, these results prompted an analysis of the internal medicine subspecialty pipeline in more detail. Fellowships typically follow completion of a three-year residency and offer additional training. Internal medicine residents who pursue these programs often specialize in fields such as cardiology, hematology/oncology or pulmonary disease.
Background
The 2026 appointment year was the largest in the history of the National Resident Matching Program (NRMP) Specialties Matching Service (SMS®), encompassing 6,606 program tracks offering 15,358 fellowship positions across 81 subspecialties, an increase of 738 positions (5.0%) from 2025.2 Of those positions, 12,963 (84.4%) were filled. There were 15,846 active applicants across all fellowships, an increase of 1,013 (6.8%) from 2025, of whom 81.8% matched into a fellowship program.
Yet as more physicians pursue advanced training, the U.S. Health Resources and Services Administration anticipates a shortage of 141,160 full-time physicians by 2038, including a primary care shortfall of 70,610.3,4 Non-metropolitan areas, where supply is already limited, are expected to see the widest gaps.5
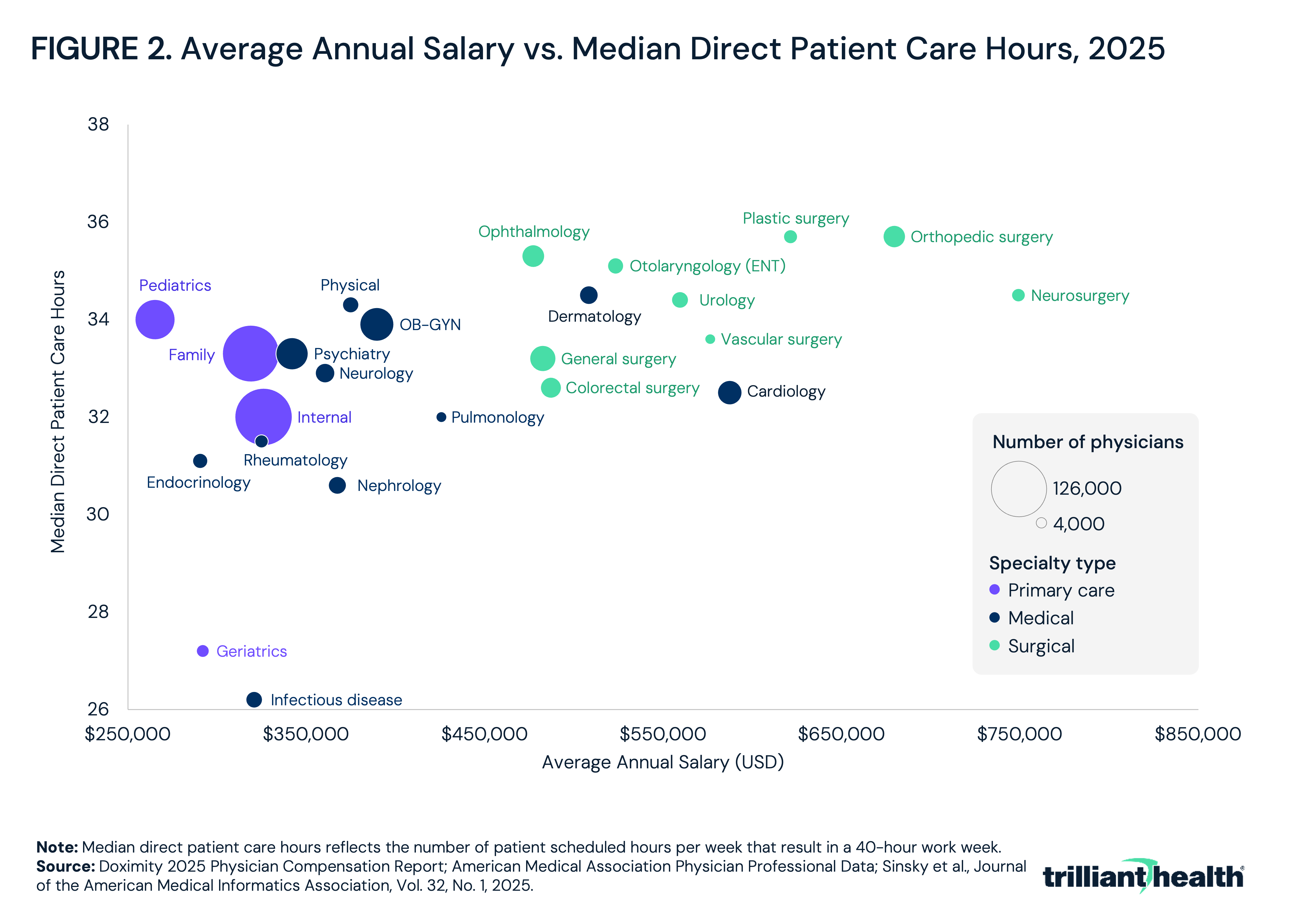
Beyond a constrained medical school pipeline relative to projected demand, financial misalignment and infrastructure disparities (e.g., low wages and limited incentives, misalignment between medical education and employment needs or a lack of long-term workforce planning in rural settings) underlie physician workforce distribution. This is especially evident in the modest return on investment for primary care training, given the high cost of medical education and long-term student debt. Primary care physicians consistently rank among the lowest-paid specialties, with average annual salaries trailing specialty physicians by more than $100,000 (Figure 2). Despite the pay gap between primary care physicians and specialists narrowing by 13% since 2022, it remains substantial.6 Notably, surgical specialists earned 87% more than primary care providers, on average, in 2024. Some primary care subspecialties saw modest gains, including preventive medicine (10.0%) and family medicine (6.0%), but these increases have not offset the financial calculus that likely contributes to physicians pursuing specialty training.
At the same time, the primary care training environment is increasingly characterized by shifting expectations and financial risks, with a growing preference for employed practice models. Fewer internal medicine physicians remain in private practice, citing unsustainable payment rates, infrastructure costs and administrative burden.7 In pediatrics, lower reimbursement rates relative to adult or procedural specialties have made it harder to recruit and retain physicians.8 Meanwhile, rural health infrastructure continues to erode as 108 rural hospitals have closed completely, and 88 have ended inpatient services since 2005, with 51 rural hospitals shifting to emergency-only care.9,10 As of May 2026, 294 rural hospitals are at immediate risk of closing, and another 720 are financially vulnerable to closure.
Compounding these challenges are new structural forces shaping where and how physicians train. One example is program signaling – a rapidly adopted feature of residency and fellowship applications – which allows applicants to express targeted interest in select programs. Top signaling factors include geographic preference, career alignment and proximity to family.11 While this system benefits applicants, it may exacerbate a geographically uneven distribution of physicians. In 2025, 25.9% of U.S. counties are fully designated primary care shortage areas, 65.4% are partially designated and 8.7% report no shortage designation.12
As internal medicine subspecialty programs expand to meet growing resident demand, understanding which subspecialties are gaining traction and which remain persistently overlooked will shape future workforce alignment, access to specialty care and the geographic distribution of physicians.
Analytic Approach
Datasets from the Main Residency Match (2015-2023) and Specialties Matching Service® (2018-2026) were analyzed to assess physician training and subspecialty trends. Fellowships include cardiovascular disease, critical care medicine, endocrinology, diabetes and metabolism, gastroenterology, geriatric medicine, hematology and oncology, hospice and palliative medicine, infectious disease, nephrology, pulmonary disease and critical care medicine, rheumatology and sleep medicine.
For subspecialty comparisons, percent changes were calculated between 2022 and 2026 to reflect the addition of new fellowships in 2022. Fill rate changes were evaluated across internal medicine subspecialties using the 2026 NRMP Results and Data report. Limitations include the inclusion of non-internal medicine applicants in some fellowships, gaps between residency and fellowship enrollment and lack of data distinguishing hospitalist from outpatient internal medicine practice.
Findings
The share of internal medicine residents pursuing specialty training has steadily increased from 61.0% in 2018 to 64.5% in 2025, peaking at 68% in 2022 (Figure 3). This consistent trend of a majority of internal residents pursuing fellowships suggests a sustained preference to pursue further specialize, despite the continuing primary care shortage.
Fill rates across internal medicine subspecialties in 2026 remain uneven, and position volume ranges from 233 positions in critical care medicine to 1,347 in cardiovascular disease. The highest fill rates are observed in cardiovascular disease (100.0%), hematology and oncology (99.5%) and gastroenterology (99.5%) (Figure 4). These three fields also rank among the largest by position volume, with cardiovascular disease growing from 1,152 filled positions in 2023 to 1,347 in 2026, hematology and oncology from 706 to 805 and gastroenterology from 656 to 755. Pulmonary disease and critical care medicine at 98.8% with 834 filled positions, rheumatology at 99.0% with 299 positions and endocrinology, diabetes and metabolism at 97.7% with 389 positions were also nearly filled. In contrast, geriatric medicine had the lowest fill rate in 2026 at 38.9%, filling just 151 positions despite 388 offered, followed by infectious disease at 60.9% with 272 filled of 447 offered and nephrology at 66.5% with 333 filled of 501 offered. Notably, all three fields saw absolute declines in the number of filled positions between 2023 and 2026: geriatric medicine fell from 177 to 151 filled positions, infectious disease from 328 to 272 and nephrology from 359 to 333, even as position capacity expanded.
Geographic variation in fellowship fill rates in 2026 reveals substantial state-level gaps, particularly in fields already struggling to attract trainees. Geriatric medicine fill rates ranged from 16.7% in Virginia to 76.5% in Massachusetts, with Ohio at 19.1%, Michigan at 23.1% and Rhode Island at 20.0% among the lowest-filled states (Figure 5). Alaska, Arkansas, Idaho, Indiana, Iowa, Kentucky, Louisiana, Montana, North Dakota, Oklahoma, Wyoming and several other states did not offer geriatric medicine fellowship positions. Nephrology fill rates ranged from 22.2% in New Jersey to 100.0% in Arizona, Nebraska and Washington, with more than half of reporting states filling fewer than 75.0% of positions, including Missouri at 50.0%, Virginia at 44.4% and Wisconsin at 42.9%. Hospice and palliative medicine ranged from 33.3% in Oklahoma to 100.0% in Alabama, Connecticut and Oregon, with Florida at 46.7% and Missouri at 50.0% among the lowest-filling larger states.
Even in subspecialties with strong fill rates, state-level variation signals geographic variability. Cardiology fill rates ranged from 72.7% in Arkansas to 100.0% across multiple states, and hematology and oncology fell below 80.0% in Iowa, Kentucky, Mississippi, Oklahoma and Wisconsin. Endocrinology, diabetes, and metabolism filled at 80.0% in Nebraska, Ohio and West Virginia despite 100.0% fill rates in most other states. Alaska, Idaho, Montana and Wyoming did not have fellowship positions across the majority of internal medicine subspecialties, leaving residents in those states with no in-state training pathway regardless of specialty interest.
Conclusion
The analysis highlights the continued trend of internal medicine residents subspecializing, with rates increasing from 61.0% in 2018 to 64.5% in 2025, peaking at 68.0% in 2022. Even as the number of available fellowship positions has grown year-over-year, demand remains concentrated in specialties offering higher compensation, fewer hours and higher reported job satisfaction (e.g., perceived pay fairness, clinical autonomy and workload manageability). The correlation between fill rate and compensation is notable, as the three highest-filling subspecialties in 2026 (i.e., cardiovascular disease, hematology and oncology and gastroenterology) are among the highest-paying fields in medicine, while the three lowest-filling (i.e., geriatric medicine, infectious disease and nephrology) consistently rank among the lowest. Geriatric medicine, which filled just 38.9% of its positions in 2026, reports an average annual compensation of approximately $292,000 – less than half the average for cardiologists. Infectious disease and nephrology follow a similar pattern, with both fields seeing declining filled position counts even as offered positions grew over the same period.
The data suggest that the physician training pipeline is not simply failing to keep pace with population health need; rather, it is actively being shaped away from it by a reimbursement structure that systematically undervalues the fields most critical to an aging and chronically ill population. The relative value unit (RVU)-based compensation system, which rewards procedural volume over care coordination, cognitive complexity and longitudinal patient management, creates financial signals that are directly reflected in fellowship fill rates. Until compensation more accurately reflects the scope and social value of generalist and aging-focused care, trainees will continue to make economically rational decisions that collectively produce irrational workforce outcomes.
In 2026, the SMS® reported 2,395 unfilled positions across 1,613 unfilled programs, representing 15.6% of all fellowship positions – signaling that applicant interest is disproportionate across subspecialties and that system-level fill rates mask widening gaps in high-need fields. The geographic aspect of this misalignment compounds the problem further. A handful of states did not offer fellowship positions across most internal medicine subspecialties, and more than a dozen states did not offer geriatric medicine positions, meaning the training pipeline in the fields most critical to an aging population is not only underfilled nationally but absent in large portions of the country.
Resident aversions to low-filling fields are compounded by worsening financial challenges – including Medicare reimbursement cuts – mounting workload concerns and burnout risk, deterring trainees from pursuing some of the very fields with the greatest population health need. Burnout rates among primary care and generalist physicians already rank among the highest of any specialty, and the fields experiencing the steepest fellowship fill rate declines between 2023 and 2026 are disproportionately those with the lowest compensation, the highest administrative burden and the fewest procedural revenue opportunities under current reimbursement structures. Research supports the connection between compensation and retention. In a survey of 2,263 physicians, those who perceived their compensation as fair had nearly 5x greater odds of work satisfaction and more than twice the odds of remaining in their current practice, with most associations between absolute compensation level and these outcomes becoming non-significant once pay fairness perceptions were accounted for.13
As of mid-2026, neither chamber has advanced the legislation beyond introduction. If enacted, the success of the legislation would depend on how strategically new positions are allocated. Expanding residency capacity in fields that are adequate or over-supplied does little to address the pipeline failures in geriatric medicine, infectious disease and hospice and palliative medicine.
Without restructuring the RVU-based compensation system to more accurately reflect the complexity, coordination demands and population health value of generalist and aging-focused care, other reforms (e.g., graduate medical education funding, residency expansion and expanded preventive care coverage) will offer only partial and temporary relief. The fill rate data make the mechanism difficult to ignore. Specialties that generate procedural revenue fill at or near 100%, while fields defined by cognitive complexity, care coordination and longitudinal patient management fill at 39%, 61% and 67%. That pattern is not a coincidence. Rather, it is a predictable output of a payment system that has never been designed to value the work of keeping complex, aging patients out of hospitals. Addressing the subspecialty pipeline requires confronting that structural reality directly, not routing around it.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
