























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
- In the 2026 National Resident Matching Program®, there were 44,344 available positions, up 2.6% from 2025.
- Primary care residencies were disproportionately unfilled in 2026 – family medicine went 16.4% unfilled, followed by pediatrics and internal medicine, 5.6% and 4.6%, respectively.
- From 2022 to 2026, vascular surgery (31.0%), neurology (23.6%), psychiatry (22.9%) and internal medicine (17.9%) saw the highest increases in residency positions offered.
Inadequate physician supply is a persistent challenge in the U.S. healthcare system. By 2038, physician supply is projected to meet 88% of demand but varies significantly by specialty. For example, primary care adequacy is projected at 80% and adult psychiatry at just 50% by 2038, while neurology is projected to exceed demand at 104% supply adequacy.1 As these workforce pressures intensify, the results of the annual National Resident Matching Program® (NRMP), referred to as “the Match," provide foundational data needed to understand the changing U.S. physician workforce and foreshadow the future composition of medical and surgical specialties.
Background
The physician workforce is shaped by several factors, including the number of medical school applications and acceptances, residency positions and the exit or retirement of existing physicians. As of 2021, 46.7% of physicians were over age 55, meaning nearly half of the workforce will reach retirement age by 2031. Furthermore, a study found that 43% of physicians changed jobs during the COVID-19 pandemic and 8% retired.2 These exits and retirements will disproportionately impact primary care and pediatrics, which have a disproportionately older workforce.3
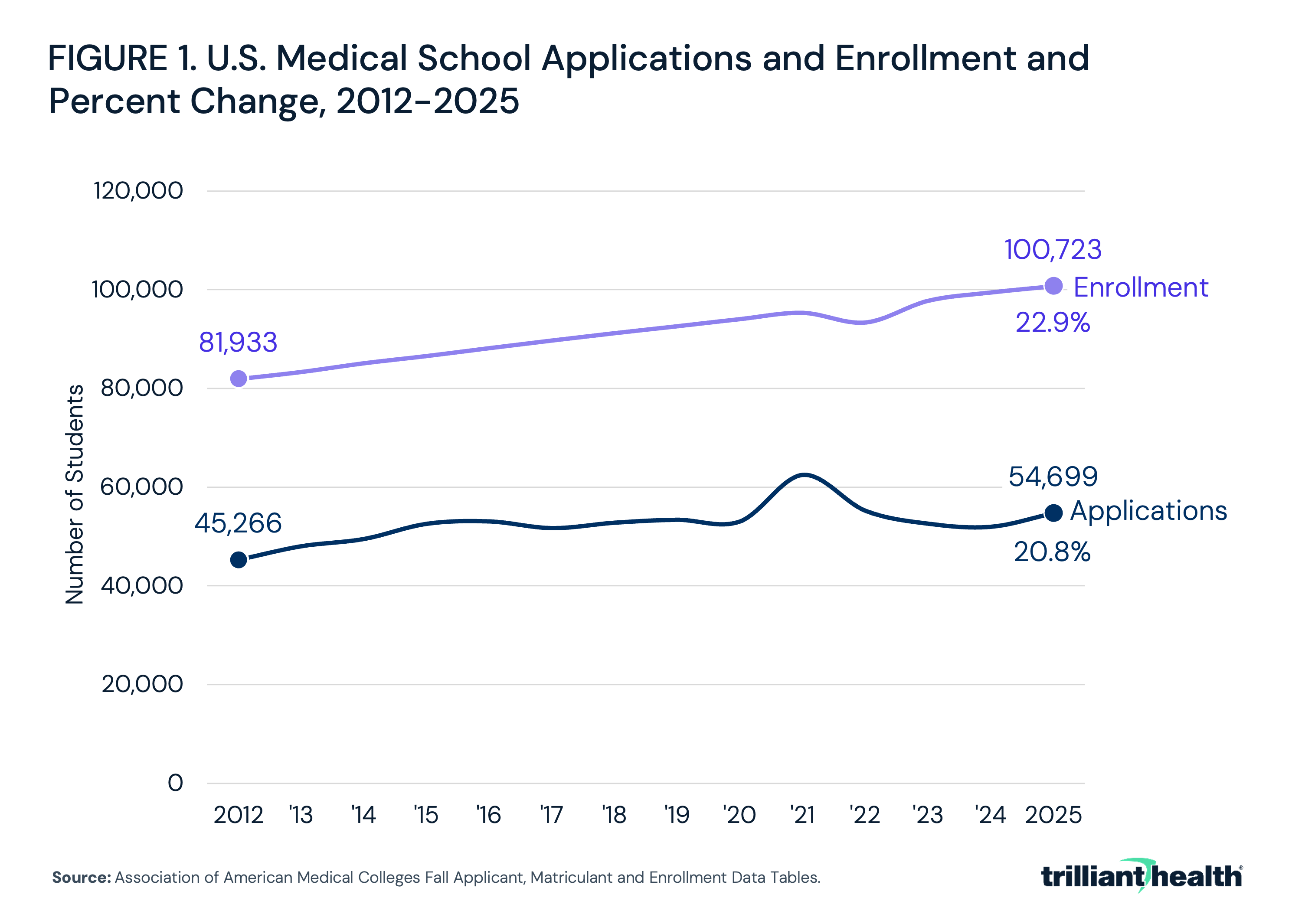
On the other hand, the 20.8% increase in medical school applications and 22.9% increase in medical school enrollment since 2012 can potentially offset these retirements to some degree (Figure 1). Between 2024 and 2025, applications grew 5.3% compared to enrollment growth of 1.3%, marking the first time in recent years that application growth outpaced enrollment – a potentially encouraging signal for the physician workforce shortage. In addition, at least eight new medical schools began enrollment or were announced to open in 2026 or 2027.4 However, training capacity expansion has been impeded by the Federal cap on Medicare-funded residency positions, which has remained largely unchanged since 1997 and has been largely outpaced by medical school enrollment.5
Even as medical school enrollment grows, the geographic distribution of training and residency programs remains a persistent challenge. As of 2024, only 14.3% of residency programs are in rural locations, and there is little evidence that Federal programs designed to incentivize physicians to practice in rural and underserved areas have had a meaningful impact.6 Since the introduction of Health Professional Shortage Area (HPSA) designations, the program has had limited measurable impact on improving physician supply in underserved areas. Between 1970 and 2018, there have been no statistically significant changes in physician density or resident mortality following HPSA designation, and 73% of designated counties remained shortage areas for at least a decade after receiving the designation – suggesting that while the program identifies need, it has not consistently driven the improvements it was designed to achieve.7 Practicing medicine in a rural setting involves personal and professional tradeoffs that financial incentives may not overcome, leaving rural communities persistently underserved.8 Growth in medical school enrollment and residency positions alone is unlikely to close geographic gaps in physician supply without deliberate effort to expand training capacity in the communities that need it most.
The NRMP uses an algorithm to place medical school graduates into the preferred residency program for the applicant and program. Selecting a residency program is a multifaceted process that balances academic standing with personal and professional priorities. Applicants evaluate programs based on how their test scores and academic metrics compare to their peers, while also weighing factors such as specialty fit, work-life balance and geographic preferences – a reflection of the quality-of-life considerations that consistently rank among residents' top priorities. In a survey of medical residents, 82% rated lifestyle as “very important” when selecting a first program, followed by adequate personal time (80%), compensation (78%) and geographic location (76%).9 These priorities likely reflect broader concerns about physician wellbeing, as nearly half of physicians (45.2%) reported at least one symptom of burnout in 2023.10 While burnout rates have modestly improved in recent years, they remain higher than those of other American workers.11 A recent survey has shown that trainees assess the factors most associated with burnout when selecting a program – time pressure, lack of autonomy, chaotic work environments and organizational cultures that undermine trust between clinicians and leadership.12
The results of the 2026 Match offer a window into the forces shaping the future U.S. physician workforce. This study examines these patterns to better understand whether growth in training capacity is keeping pace with workforce demand, and where gaps in specialty and geographic distribution may persist.
Analytic Approach
National Resident Matching Program data from 2022 through 2026 were analyzed to examine match results, inclusive of post-graduate year 1 (PGY-1), post-graduate year 2 (PGY-2) and physician MD and DO applicants, including the number and percentage of unfilled residency positions by specialty. Specialties with fewer than 70 available residency positions (e.g., occupational and environmental medicine) and preliminary and transitional residency positions were excluded from the analysis.
Findings
During the 2026 Match cycle, there were 44,344 available PGY-1, PGY-2 and physician residency positions, a 65.6% increase from 2012.13 For the 2026 Match, 53,373 medical students registered, of which 48,050 submitted a certified rank-ordered match list, resulting in 41,482 matches.14 Of applicants with a certified rank-ordered match list, 79.8% matched to a first-year residency position. Despite the structured nature of the process, approximately 5-7% of U.S. medical school graduates do not match on Match Day each year.15 For these applicants, the Supplemental Offer and Acceptance Program (SOAP) provides a structured pathway to place unmatched applicants into remaining open positions.
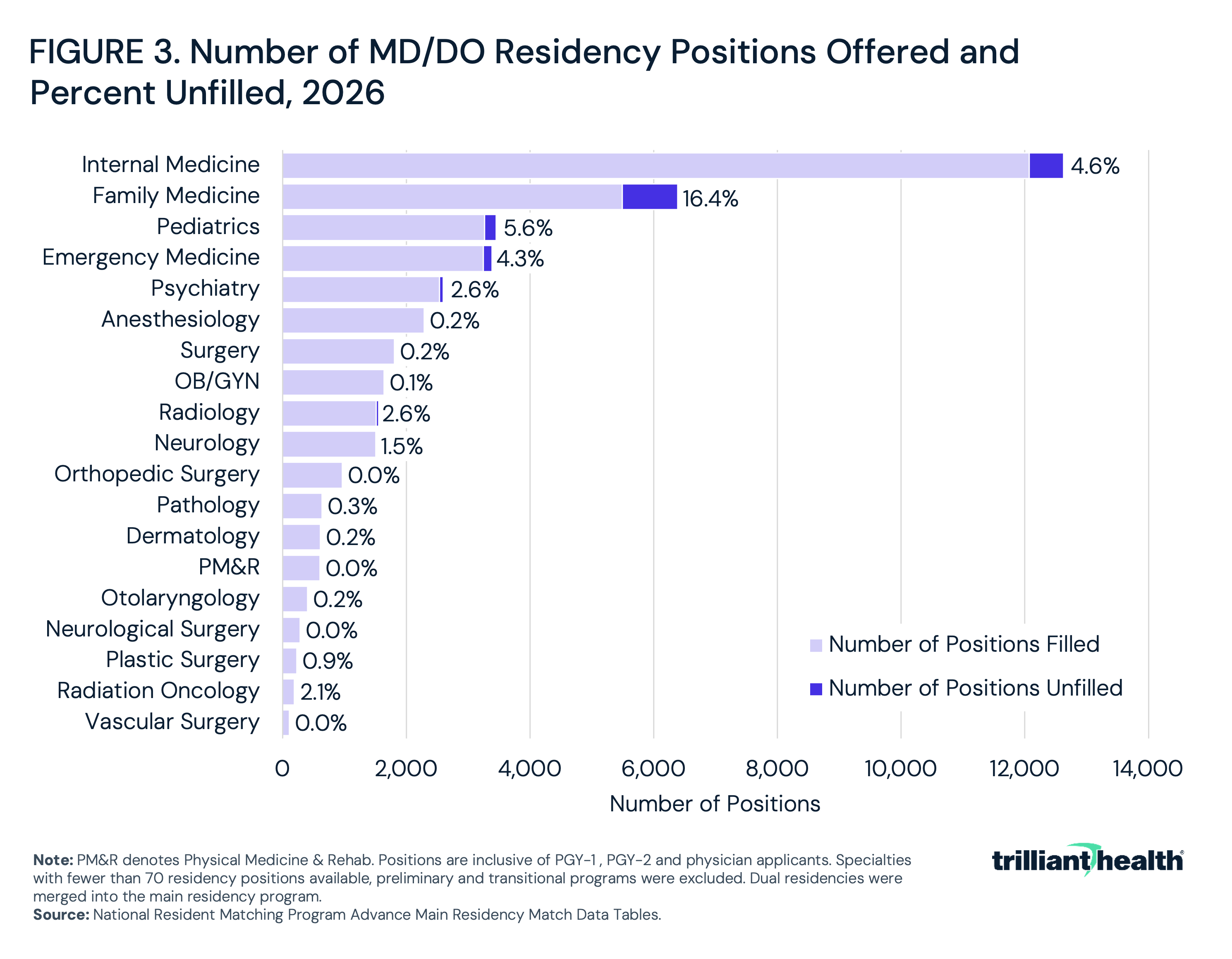
Of available positions, 47.0% were for primary care specialties – internal medicine (12,071), family medicine (5,491) and pediatrics (3,267) (Figure 2). From 2022 to 2026, the specialties with the lowest growth in positions offered were pathology, which grew just 0.8% from 631 to 636 positions, radiation oncology, up 3.0% from 166 to 171, and pediatrics, up 5.9% from 3,085 to 3,267. In the same period, the specialties with the greatest growth were vascular surgery, up 31.0% from 84 to 110 positions; neurology, up 23.6% from 1,171 to 1,447; psychiatry, up 22.9% from 2,047 to 2,516; and internal medicine, up 17.9% from 10,241 to 12,071.
As of 2026, the share of unfilled positions varies considerably across specialties. Orthopedic surgery, physical medicine and rehab (PM&R), neurological surgery and vascular surgery residencies were 100% filled in 2026. Other competitive specialties had relatively low shares of unfilled positions, such as anesthesiology (0.2%), OB/GYN (0.1%) and dermatology (0.2%). In contrast, family medicine had the highest share (16.4%) and number of unfilled positions (899), followed by pediatrics (5.6%, 184 unfilled positions) and internal medicine (4.6%, 554 unfilled positions).
Not only does family medicine have the highest share of unfilled positions nationally, fill rates at the state level reveal considerable geographic variation. In 2026, six states achieved a fill rate of 100% including Alaska, Massachusetts, Rhode Island, Vermont and Utah (Figure 4). In contrast, 12 states had a fill rate at or below 75%, with the lowest rates in New Hampshire (54.5%), Montana (66.7%) and Oregon (67.8%), suggesting that targeted state-level strategies may be needed alongside national policy efforts.
In recent years, surgical and specialized fields have maintained consistently high fill rates, with anesthesiology, general surgery, orthopedic surgery, plastic surgery, neurological surgery, vascular surgery and PM&R all at or near 100% in 2024, 2025 and 2026 (Figure 5). In contrast, the fill rate for family medicine has declined from 87.8% in 2024 to 83.6% in 2026 – the lowest of any specialty. Pediatric positions rebounded from a 91.8% fill rate in 2024 to 95.3% in 2025, before decreasing to 94.4% in 2026.
Conclusion
The 2026 Match data reflect a physician workforce pipeline that is growing in volume but not at a rate commensurate with demand and clinical need. While the number of residencies offered is increasing, supply is projected to be inadequate for most physician specialties by 2038. The specialties with the greatest growth in positions offered from 2022 to 2026 – vascular surgery (31.0%), neurology (23.6%), psychiatry (22.9%) and internal medicine (17.9%) – are each still projected to face supply shortfalls by 2038, with the exception of neurology, which is projected to reach 104% supply adequacy by 2038.16 This pattern suggests that residency expansion is being driven as much by economic incentives and trainee lifestyle preferences as by population health need.
Given the near-universal belief in the importance of primary care focused care models, the decline in primary care fill rates is concerning. Within primary care, internal medicine added 283 positions from 2025 to 2026 (11,788 to 12,071), though its fill rate dipped slightly from 96.8% to 95.4% in 2026. Family medicine is more concerning – despite modest growth in positions offered (5,357 in 2025 to 5,491 in 2026), its fill rate has declined from 87.8% in 2024 to 83.6% in 2026, the lowest of any specialty. This pattern within primary care – growing capacity that is going increasingly unfilled – is particularly notable given projections that primary care supply will only meet 80% of demand by 2038. The data suggests that simply expanding training capacity is insufficient. The vulnerability of rural and primary care pipelines is further exposed by recent increases in H-1B visa fees, which threaten to reduce the supply of international medical graduates who make up 25% of the U.S. physician workforce and disproportionately practice in shortage specialties and underserved communities.17
The persistence of unfilled positions in primary care, pediatrics and emergency medicine – specialties that serve as the foundation of accessible, community-based care – raises important questions about the long-term sustainability of the U.S. healthcare system. These pressures are unfolding against a backdrop of a growing and aging patient population with increasingly complex health needs. As trainees increasingly weigh burnout risk, work-life balance and organizational culture in their program selection, specialties that have not meaningfully addressed these concerns are likely to face continued recruitment challenges. The widening gap of primary care physicians creates a concerning feedback loop: a shrinking primary care workforce may lead to greater dissatisfaction and distrust in the healthcare system, which discourages patients from seeking care. Increasing the number of available residency positions among primary care and frontline positions has not materially improved the growing supply gap, necessitating novel approaches in improving provider supply.
Given the significant compensation gaps between primary and specialist care - evidenced by the average pediatrician compensation of $266,000 in 2025 and compared to the average orthopedic surgeon compensation of $611,000 – it is unsurprising that many physicians make economically rational decisions in their choice of specialty.18 The question for policymakers – particularly Congress – is the reluctance to reimburse primary care at levels commensurate with its supposed clinical importance.
Instead of addressing the fundamental compensation issue, policymakers have often focused on somewhat less controversial approaches to address the primary care shortage, such as expanding the role of allied health professionals – including nurse practitioners and physician assistants. Between 2019 and 2023, the share of U.S. healthcare visits delivered by non-physicians rose from 14.0% to 25.6%, reflecting a meaningful shift in how primary care is being delivered.19 However, primary care practices face growing competition for allied health professionals from specialty practices in fields such as dermatology and cardiology, which can offer more competitive salaries and workloads – limiting how far this approach can go in closing the gap.
Addressing these trends requires more than incremental increases in residency positions and miniscule annual adjustments to the Medicare physician fee schedule. Evidence supports targeted strategies – recruiting and training physicians in the regions where they are most needed, expanding rural and community-based residency capacity and reforming reimbursement structures that currently disadvantage primary care relative to procedural specialties.20 While the 2025 uptick in medical school applications relative to enrollment is an encouraging signal for the long-term pipeline, the 2026 Match data suggests that sustaining this trend will require progress on the structural and cultural barriers that continue to steer trainees away from the specialties and communities that need them most.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
