























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Study Takeaways
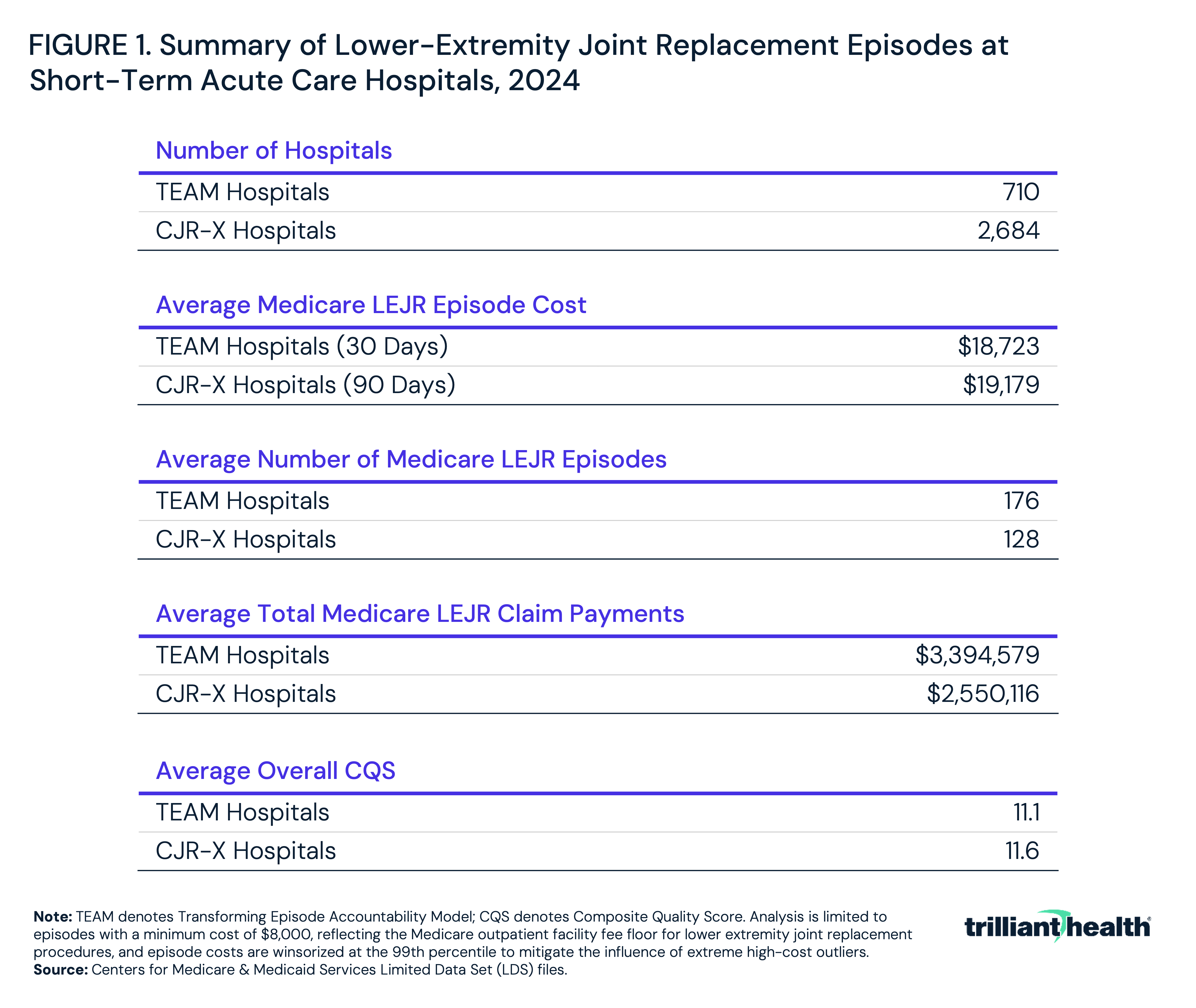
- In 2024, TEAM hospitals had average 30-day lower-extremity joint replacement (LEJR) episode costs of $18,723, and CJR-X hospitals had average 90-day LEJR episode costs of $19,179.
- There is no observable correlation (r=-0.1) between LEJR episode cost and quality, suggesting that lower-cost episodes do not correspond to better quality, and vice versa.
On January 1, 2026, the Centers for Medicare and Medicaid Services' (CMS) Transforming Episode Accountability Model (TEAM) commenced, under which 721 hospitals are required to accept financial accountability for five surgical service line categories, including lower-extremity joint replacement (LEJR). Under TEAM, the surgical episode includes both the hospital-based costs for the procedure and the post-acute care for 30 days post-discharge.
On April 10, 2026, CMS issued the FY 2027 Hospital Inpatient Prospective Payment Systems (IPPS) proposed rule, which included a provision that would require every short-term acute care hospital not already participating in TEAM to accept financial accountability for the total cost of LEJR episodes (the surgical care and post-acute care for 90 days post-discharge) for Traditional Medicare beneficiaries.1
If the FY 2027 IPPS rule is finalized as proposed, the Comprehensive Care for Joint Replacement Expanded (CJR-X) model would take effect October 1, 2027. Together, TEAM and CJR-X would make episode-based payment the universal reimbursement structure for hospital-based LEJR under Traditional Medicare – a policy shift with no precedent since 1965 when Medicare was established.2,3
Background
Since the introduction of Diagnosis Related Groups (DRGs) in 1983, Medicare hospital reimbursement has been prospective, meaning a fixed payment per discharge to reimburse a hospital for all costs incurred from admission through discharge. In a prospective payment system, hospitals generate margin by delivering care during the inpatient stay at a cost lower than the applicable DRG rate but bear no financial accountability for costs incurred by a patient after the hospital discharge. The combination of financial incentives under prospective payment and technological advances has resulted in the decline in the average length of stay for total hip arthroplasty from 3.0 days in 2012 to 1.1 days in 2023.4
In contrast to hospital-based care, CMS reimburses post-acute care providers under separate fee-for-service payment systems. In the absence of prospective payment for post-acute care, post-discharge utilization following LEJR has remained highly variable. Patients recovering from LEJR may be discharged to any combination of inpatient rehabilitation facilities, skilled nursing facilities or long-term care hospitals or alternatively referred to home health agencies or outpatient therapy clinics.
Since 2012, CMS, through its Centers for Medicare and Medicaid Innovation (CMMI), has sought to address the wide variation in post-acute utilization and associated costs through voluntary bundled payment models, including Bundled Payments for Care Improvement (BPCI) and Comprehensive Care for Joint Replacement (CJR).5,6 Voluntary participation has tended to attract providers already positioned to perform well under a given model's financial terms, limiting the extent to which reported savings reflect behavioral change rather than favorable selection. Net savings generated by CMMI models from 2012 through 2025 across bundled payment, accountable care and primary care transformation programs have been modest relative to total Medicare spending and have not produced a measurable reduction in Medicare's aggregate spending trajectory over the same period.7 Performance data also show that operational costs associated with model administration have offset a meaningful share of reported gross savings in several programs.
Under the proposed CJR-X model, individual providers and suppliers providing LEJR care during the episode would continue to be paid under existing Medicare payment systems. Financial reconciliation would occur at the hospital level following the end of each performance year, when actual total episode spending would be compared to the hospital's target price. Hospitals that exceed their target price, net of quality performance adjustments, would be required to repay a portion of episode spending to CMS. Hospitals bearing repayment liability will face pressure to reduce post-acute utilization and unit costs across every provider type involved in LEJR recovery. This structure will likely prompt hospitals to prioritize post-acute network development and referral management programs.
As with TEAM, CMS's stated goals for the CJR-X model are to encourage hospitals to work collaboratively with physicians and post-acute providers to support patients, coordinate care across settings through the recovery period and reduce unnecessary or duplicative services, including avoidable hospital readmissions.8 Together, TEAM and CJR-X would be the first mandatory payment model applied to all U.S. hospitals performing a single procedure, a significant departure from the voluntary participation structure of most CMMI models.
This study examines the distribution of total episode cost and quality across hospitals subject to TEAM and CJR-X based on 2024 LEJR volumes, characterizes the post-acute care landscape that drives episode cost variance and considers the implications for hospitals and the broader set of health economy stakeholders downstream of the LEJR episode.
Analytic Approach
This analysis leveraged 2024 CMS Limited Data Set (LDS) claims to examine Traditional Medicare LEJR episode cost and quality performance for every hospital performing LEJR, whether now participating in TEAM or included in the proposed CJR-X model. LEJR episodes were identified using the MS-DRGs 469, 470, 521 and 522 for inpatient procedures and HCPCS codes 27130, 27447 and 27702 for hospital-based outpatient procedures. For each hospital included in the proposed CJR-X model, 90-day episode costs were calculated following discharge or the date of an outpatient procedure. Episode costs include spending on care rendered across inpatient, hospital outpatient, long-term acute care (LTAC), skilled nursing facility (SNF), home health, hospice and emergency department settings during the 90-day window. Ambulatory care, anesthesia, professional fees and durable medical equipment (DME) costs are not included in these episode cost calculations. Actual total episode costs are therefore higher than those reported here.
Quality performance was assessed using the Overall Composite Quality Score (CQS) consistent with the CJR-X proposed rule. Hospitals were assigned to one of four quality categories based on their CQS: Below Acceptable (below 5), Acceptable (5 to 6.9), Good (6.9 to 15), and Excellent (above 15). Episode cost and quality distributions were analyzed at the Core-Based Statistical Area (CBSA) level, hospital level and the patient level to characterize variation in cost and quality.
Findings
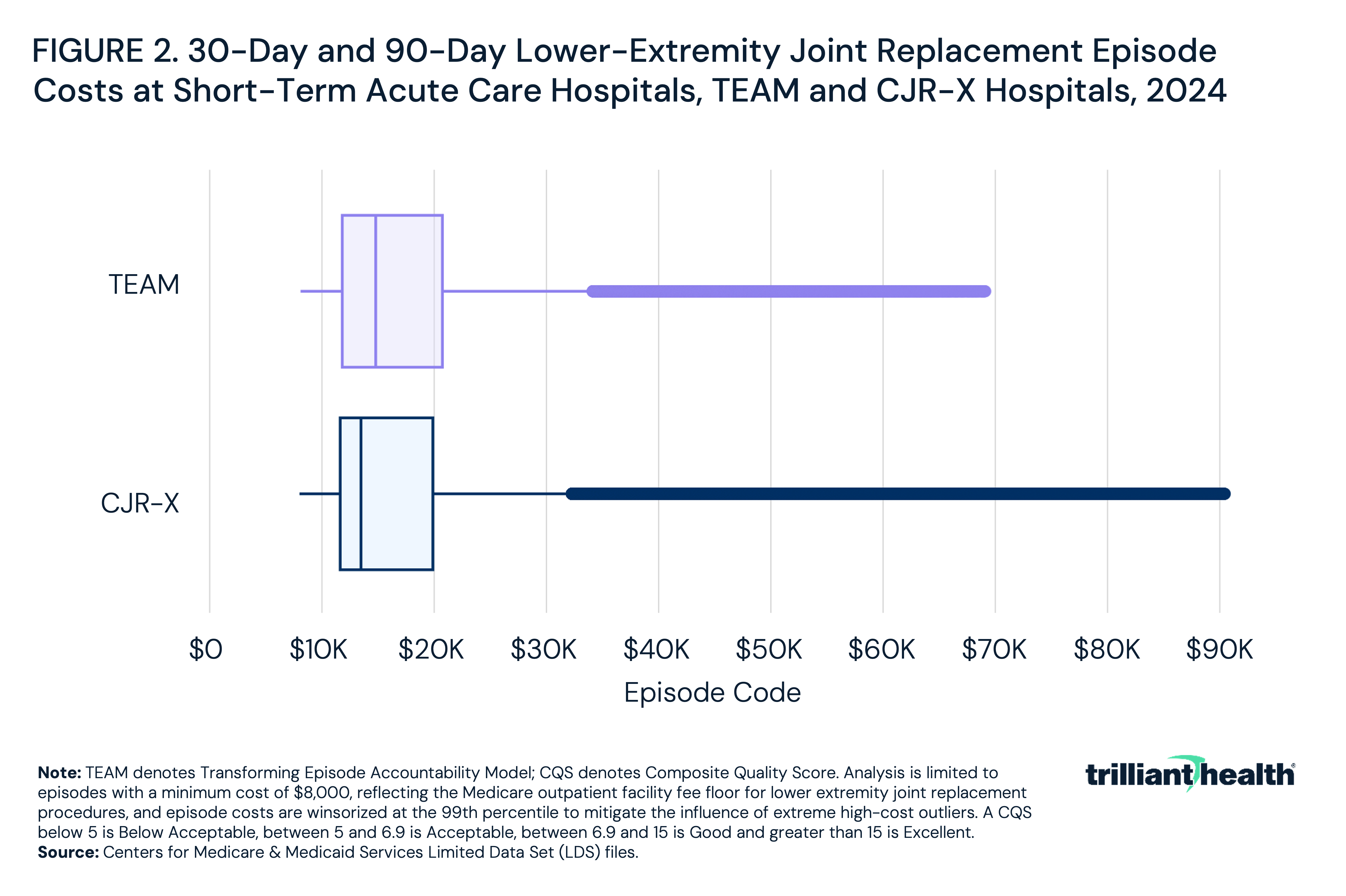
In 2024, TEAM hospitals had average 30-day LEJR episode costs of $18,723, and CJR-X hospitals had average 90-day LEJR episode costs of $19,179 (Figure 1). The range of episode costs for CJR-X is wider than TEAM hospitals (Figure 2). TEAM hospitals had a greater average number of Medicare LEJR episodes than non-TEAM hospitals (176 compared to 128) and, in turn, higher average total Medicare LEJR reimbursement ($3.4M for TEAM hospitals and $2.6M for non-TEAM hospitals). Quality performance was comparable, with an average CQS score of 11.6 for non-TEAM hospitals and 11.1 for TEAM hospitals.
In 2024, 46.7% of hospitals fell in the Good CQS category, followed by those in the Acceptable category at 40.2%, Below Acceptable at 8.2% and Excellent at 4.9% (Figure 3). Despite this distribution, median episode costs were relatively comparable across CQS categories. Hospitals in the Excellent category had the lowest median episode cost at $13,869 and the narrowest interquartile range, from $12,577 to $16,427. Hospitals in the Good category had a median episode cost of $17,097 with an interquartile range spanning $14,380 to $22,064. Hospitals in the Acceptable and Below Acceptable categories had the highest median costs at $18,693 and $19,308, respectively.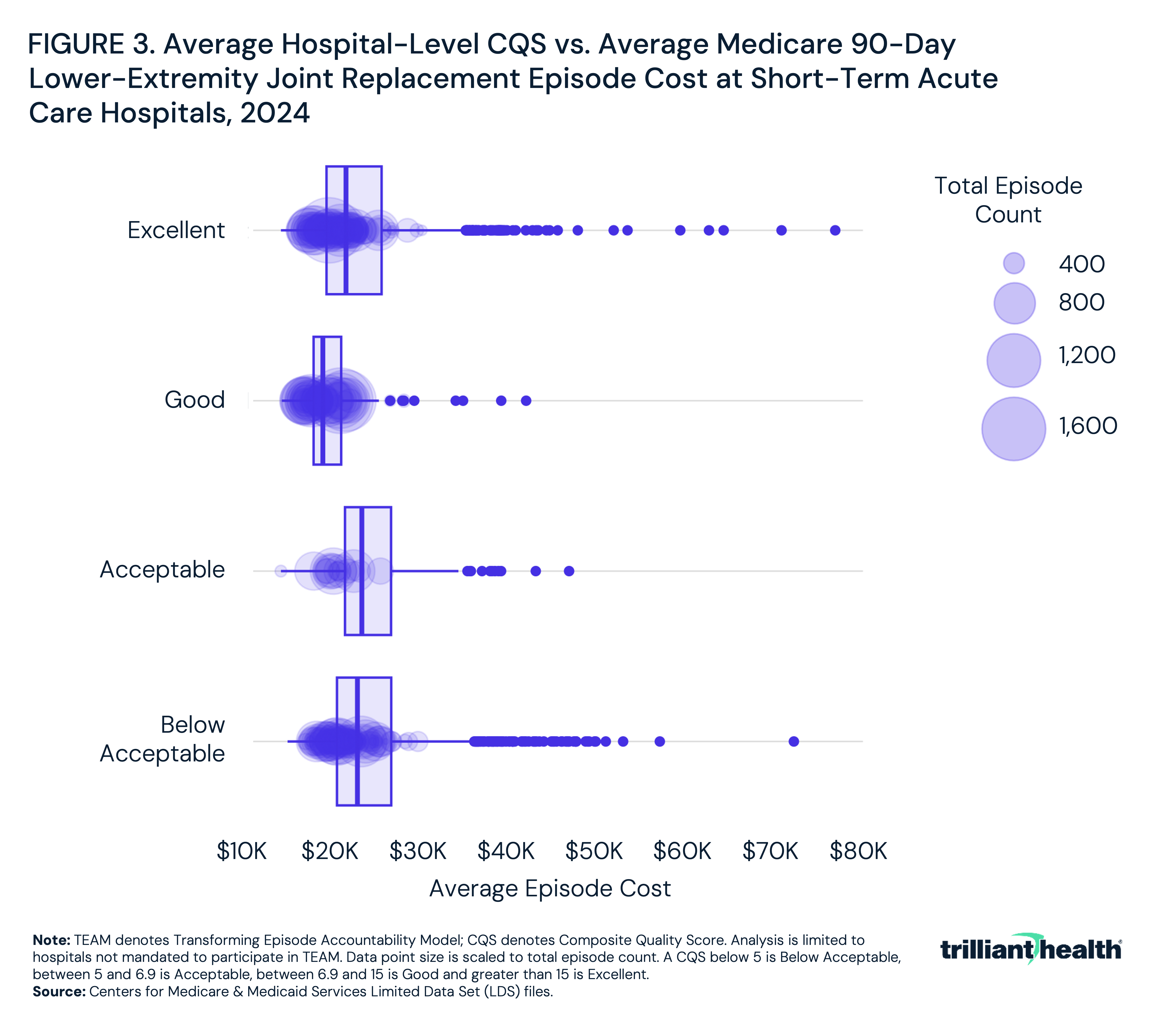
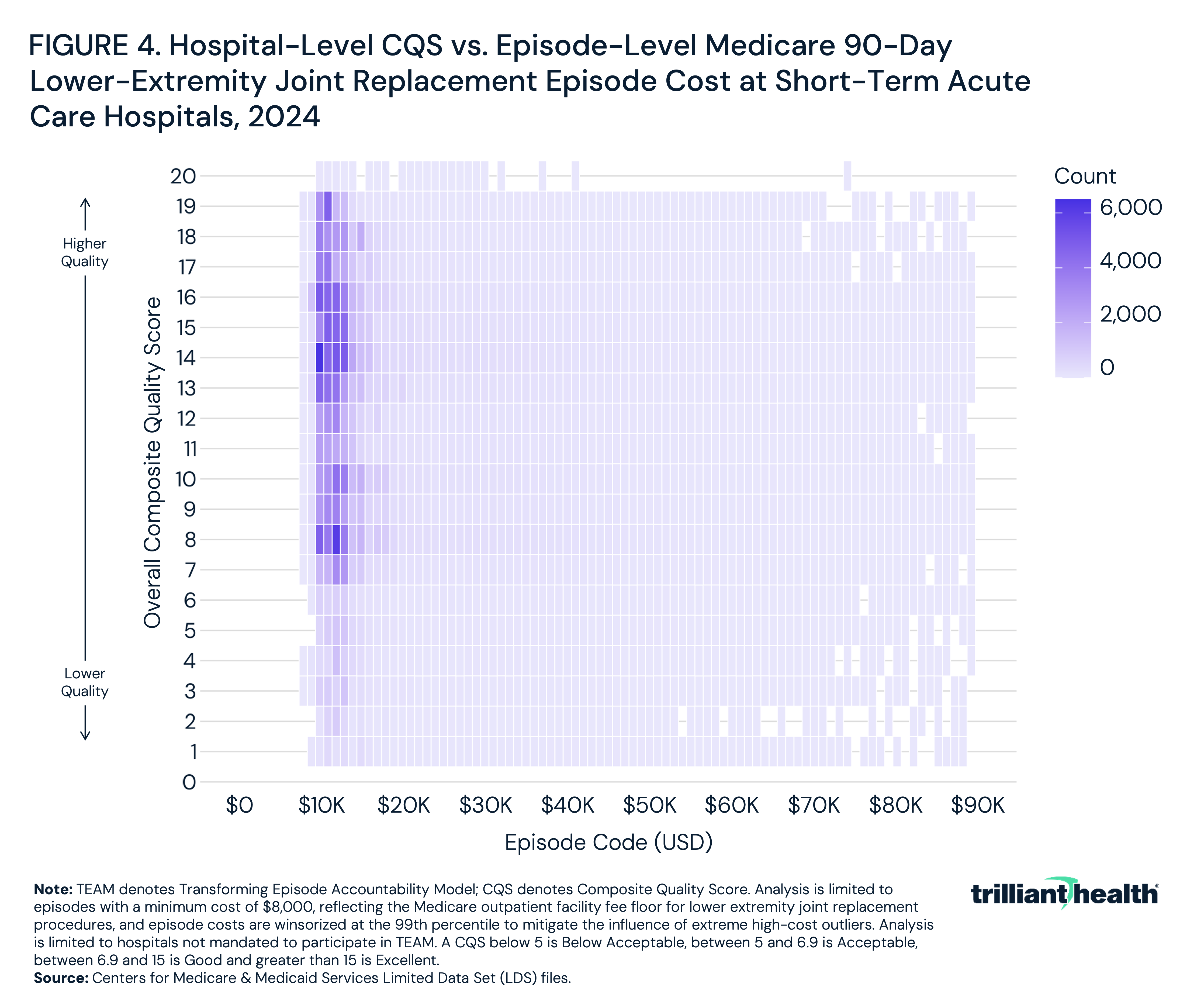
At the episode level, Medicare 90-day LEJR episode costs varied widely with an average cost of $19,179 (Figure 4). Across all four CQS categories, high- and low-cost episodes were present, and there is no observable correlation (r=-0.1) between episode cost and CQS at the patient level. Notably, episodes with CQS values in the Excellent range included the lowest- and highest-cost episodes, suggesting that lower-cost episodes do not correspond to better quality, and vice versa.
Conclusion
TEAM and CJR-X represent CMS's most direct acknowledgment yet that the variance in utilization of post-acute care is the root cause of significant variance in the cost of longitudinal patient journeys for Traditional Medicare enrollees. In the absence of evidence that voluntary payment reform can reduce that variance, the proposed CJR-X model, combined with TEAM, would establish episode-based payment as the universal Traditional Medicare reimbursement structure for hospital-based LEJR. History suggests that Medicare Advantage plans would adopt that approach as well.
At the conceptual level, TEAM and CJR-X represent a material expansion of the DRG-based prospective payment system. At the operational level, TEAM and CJR-X necessitate a radical change in hospital management, particularly discharge planning. After being incentivized for 43 years to focus solely on the costs of the inpatient stay, TEAM and, as proposed, CJR-X hold hospitals financially responsible for the costs of care delivered off-campus, most of which is beyond their span of financial or operational control. Notably, Medicare Conditions of Participation and the IMPACT Act of 2014 limit the ability of hospitals to direct referrals to their own post-acute facilities, the most logical way to manage post-discharge costs.
TEAM's 30-day post-discharge accountability window captures the most acute and cost-intensive phase of recovery, but CJR-X's extension to 90 days encompasses a substantially longer period of post-acute utilization (i.e., skilled nursing, home health, outpatient therapy and physician follow-up) that is both more variable in cost and less directly related to the quality of the hospital-based encounter. For CMS to extend a hospital’s financial accountability from one or two days of an inpatient stay to 30-90 days post-discharge is a monumental change.
Our finding that there is no observable correlation between episode cost and quality at the patient level (r = -0.1) aligns with much of our prior research and suggests that variation results from post-discharge referral and utilization patterns combined with patient-specific factors. Even so, hospitals with the worst quality performance have the highest episode costs, on average, suggesting poor care coordination driving avoidable post-acute utilization. The wide variation in total episode cost observed across hospitals at current performance levels, combined with the absence of a meaningful correlation between cost and quality, suggests that while meaningful savings opportunity exists, it is distributed unevenly across hospitals, markets and post-acute referral patterns.
Notably, the January 1, 2026 effective date for TEAM corresponds to the first phase of CMS's most recent changes to the Inpatient Only (IPO) list. Total knee arthroplasty (TKA) and total hip arthroplasty (THA) were removed from the IPO list in 2018 and 2020, respectively, which catalyzed a shift of 17.9% of TKA procedures and 35.8% of THA procedures performed on Traditional Medicare beneficiaries to outpatient settings.9 Because TEAM and CJR-X apply to both hospital inpatient and outpatient settings, these models implicitly encourage further migration of care to outpatient settings. However, as LEJR procedures continue to migrate beyond the hospital outpatient department to ambulatory surgical centers, which – for now - fall entirely outside the scope of both TEAM and CJR-X, the volume of episodes subject to mandatory bundled payment will increasingly be comprised of relatively more complex, higher-acuity patients. This selection effect has direct implications for target price calibration under TEAM and CJR-X. If the LEJR population subject to mandatory bundled payment becomes systematically higher-risk over time as lower-complexity cases migrate to ambulatory surgical centers, episode costs will face upward pressure driven by patient mix rather than inefficiency. CMS's ability to distinguish between these two sources of cost variation, and to adjust target prices accordingly, will be critical to the credibility and durability of both models' financial terms.
Ultimately, TEAM and CJR-X, while described as value-based payment models, are price caps under which CMS transfers the risk of excessive post-acute care spending to hospitals, which in turn will increase pressure on device manufacturers and post-acute providers to demonstrate measurable contributions to episode quality or cost efficiency.. Those who cannot deliver value for money should expect to receive fewer referrals.
Whether mandatory episode-based payment at scale reduces the systemic costs of care depends primarily on whether hospitals can implement and manage episode costs without increased administrative costs, which the history of CMMI payment model performance suggests is unlikely. Whether commercial insurers will follow CMS’s lead to transfer the risk of excessive post-acute care spending to hospitals is something that history suggests is highly likely.
Get the latest insights delivered to your inbox.
Was this shared with you?
Subscribe for weekly insights.
Subscribe to receive weekly insights from Trilliant Health's Research Team
Interested in citing our research? Please follow this guide.
