























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Counterpoint
Hal Andrews | April 4, 2023Last week, Nashville hosted ViVE, a conference which promotes itself as “the fresh, new way to think about the business of healthcare” but whose content focuses on decades-old concepts like care coordination, telehealth and interoperability. In private conversations, several attendees admitted their steadfast commitment to incrementalism, which every rational participant in a negative-sum game should have.
While marveling at the “investment” required to attend, sponsor an event or host a booth at ViVE by those prone to lament the “waste” in healthcare, I asked myself this question:
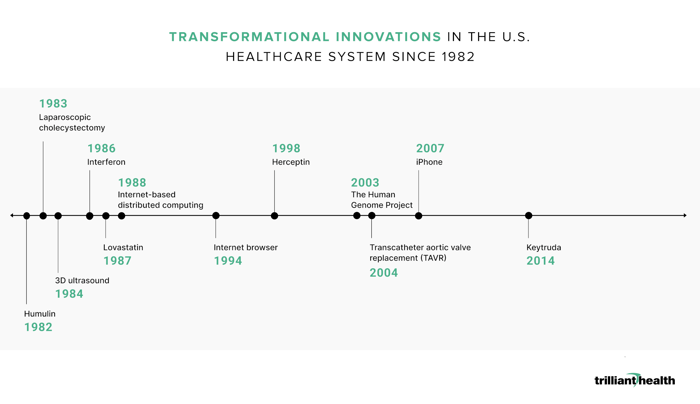
What are the real innovations in the health economy in the past 40 years, and how many of those were transformational?
Only three came immediately to mind: laparoscopic cholecystectomy, which inaugurated the utilization of minimally invasive surgical techniques, the Human Genome Project and Keytruda. Believing that there must have been more than three transformational healthcare innovations in the past 40 years, I solicited thoughts from a small group of colleagues to compile the following list:
Several colleagues also mentioned electronic medical records as a transformational innovation. I agree that digitization – of documents, music and video – was both innovative and transformational. In 1986, I was in the studio with the legendary Jimmy Bowen when he recorded the first digital album in the history of Music City. Unlike the healthcare industry, the transformation of the U.S. entertainment industry from analog to digital was not sponsored by the Federal government.
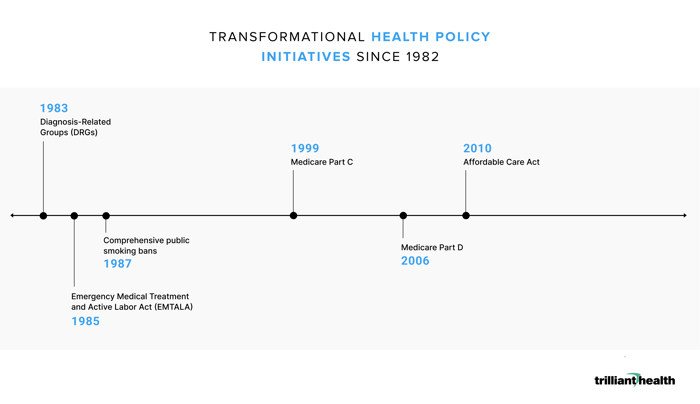
Interestingly, several colleagues also cited the following policy initiatives as both innovative and transformational:
Who Isn’t Leading Transformational Innovation
To consider that over the last 40 years the Federal government has been the leading “change agent” within the U.S. healthcare system is, perhaps, a teachable moment for the self-reverential and self-referential who will gather at HIMSS in a few weeks. In any event, here is the key point: nobody who attended ViVE last week – including yours truly – contributed to any of the transformational innovations cited above, although one attendee did leverage artificial intelligence and distributed computing to reduce sepsis in a large health system, realizing Don Berwick’s famous “triple aim.” Notably, the transformational innovations listed above were created by individuals or small groups of scientists or technologists, in many cases in a previous century; none were created by a healthcare system or health insurer or financier or consultant.
Peter Drucker would not have been surprised:
Major changes always start outside an organization. A retailer may know a great deal about the people who shop at its stores. But no matter how successful, no retailer ever has more than a small fraction of the market as its customers; the great majority are noncustomers. It is always with noncustomers that basic changes begin and become significant. At least half of the important new technologies that have transformed an industry in the past fifty years came from outside the industry itself.1
(Emphasis added)
Dr. Drucker’s observation about “a small fraction of the market” is something that most health economy stakeholders have never fully embraced or even understood, but it is foundational to developing innovative strategies. Dr. Drucker also noted that “predicting the future can only get you in trouble.” Instead, he emphasized the “anticipation of a future that has already happened” by “finding and exploiting the time lag between the appearance of a discontinuity in the economy and society and its impact.”2
Transformational Innovation vs. Financial Engineering
Much of what has passed for “transformation” in the U.S. health economy in the past 40 years is, in fact, a small group of people skilled in “finding and exploiting the time lag between the appearance of a discontinuity” in healthcare policy. The innovation that transformed Nashville’s economy was the realization in 1968 by a small group of physicians that applying Holiday Inn’s standard design within a cost-based reimbursement system provided first-mover advantage to develop new hospitals in Sunbelt states. Similarly, Medicare Part D transformed Humana’s business in the past 20 years, even if since its founding as a nursing home operator Humana’s key customer has always been the Federal government.
Transformation and innovation implicitly originate in a desire to change the status quo, usually driven by fear or greed. In business, people motivated by fear or greed understand the fundamental need to compete. The people I saw at ViVE last week are seemingly content with the status quo, tacitly agreeing that talking about innovation and transformation is sufficient, using phrases like “directionally correct” and “industrial logic.”
The Septic Nature of the Status Quo
Unfortunately, just as culture eats strategy for breakfast, the status quo, one of the four horsemen of the coming healthcare apocalypse, is the silent killer of transformational innovation in healthcare. As a result, the cost of the U.S. healthcare “system” is bankrupting America. Many have written about the many flaws of the system for many years. Little has changed.
In 2004, Michael Porter and Elizabeth Teisberg wrote this about “positive-sum competition”:
For that process to begin, however, the locus of competition has to shift from “Who pays?” to “Who provides the best value?” Getting there will require changes in the strategies of providers and payers and in the behaviors of employers purchasing health plans…
Under positive-sum competition, providers would not attempt to match competitors’ every move. Instead, they would develop clear strategies around unique expertise and tailored facilities in those areas where they can become distinctive. Most hospitals would retain a wide array of service areas, but they would not try to be all things to everyone. In most businesses, it is common sense to develop products and services that create unique value. For many hospitals, developing uniqueness is a significant change in mind-set and deciding what not to do is an even more radical idea.
Prices would be posted and readily available. Providers would charge the same price to any patient for addressing a given medical condition, regardless of the patient’s group affiliation. Providers could and would set different prices from their competitors, but that pricing would not vary simply because one patient was insured by Aetna, another covered by Blue Cross, and another self-insured. Payers could negotiate, but price changes would have to benefit all patients, not just their own. The cost of treating a medical condition has nothing to do with who the patient’s employer or insurance company is…
Positive-sum competition would induce payers to compete to create value, not just to minimize cost. They would simplify billing and administrative processes. They would serve subscribers by identifying treatment alternatives and providers with excellent outcomes. They would help subscribers to know when and where it is appropriate to travel outside of their immediate areas for quality care.3
(Emphasis added)
Porter and Teisberg made several astute observations, but they failed to identify both the necessary catalyst for their view of positive-sum competition and a logical framework for the transition they championed.
The Fantasy of Value-Based Care vs. The Reality of Value-Based Competition
Value-based care, the siren call of many a consultant, academic and financier for almost two decades, is the biggest fairy tale in the health economy. Truthfully, “true” value-based care (i.e., capitation and bundles, not “quality bonuses”) has always been theoretical because of the longstanding information asymmetry between payers and providers. The proof is the continued prevalence of fee for service reimbursement throughout the health economy.
Even if value-based care were not theoretical, it would at best be a “point solution,” in industry parlance. If there is a value-based care industry in the U.S. healthcare system, it more closely resembles the “mom and pop” nature of home health agencies than the scale of a national payer. To any disinterested observer, it is obvious that value-based care is insufficient to cure the financial ills of the U.S. healthcare system. Only value-based competition can do that.
In 2004, Porter and Teisberg referred to the current healthcare system as a “zero-sum” game. If it was in 2004, it isn’t now; in 2023, healthcare is a negative-sum game.
“The most difficult problems are negative-sum situations, where the pie is shrinking. In the end, the gains and losses will all add up to less than zero. This means that the only way for a party to maintain its position is to take something from another party, and even if everyone takes his or her share of the "losses," everyone still loses in comparison to what they currently have or really need. This type of situation often sparks serious competition.”4
(Emphasis added)
The winners of healthcare’s negative-sum game will be those who compete on value most effectively, whether at the local or regional or national level. As Porter and Teisberg suggested, some will win by deciding to quit “being all things to everyone,” like Humana’s recent announcement to exit its Employer Group Commercial Products business.5
In healthcare’s negative-sum game, everything is information, and information is everything. The information required for value-based competition now exists, which means that every stakeholder is without excuse.
In turn, the opportunity to be transformational awaits all those with the requisite competitive fire – the recognition that they must compete, and the ferocity with which they do so. If you had that opportunity, would you capture it or just let it slip?
Horizontal Spacer@hubspot/horizontal_spacer18473372modulefalse{}{} Horizontal Spacer@hubspot/horizontal_spacer18473372modulefalse{}{}
1. Peter Drucker, “The Daily Drucker”
2. Ibid.
3. https://hbr.org/2004/06/redefining-competition-in-health-care