























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Counterpoint
Hal Andrews | October 4, 2023In the 1980s, a healthcare company found itself in hot water with the Securities Exchange Commission (“SEC”) for misuse of what the SEC calls “material information.” In an executive team discussion of how to respond to the SEC, one executive famously asked the group: “Do you want them to think we are stupid, or crooks?”
Over the past few months, we have disclosed numerous insights from the health plan price transparency files. After 30 years in the industry, I should not be surprised that the most common response from health economy stakeholders is “I knew that.” Based on what the health plan price transparency files reveal, anyone who had prior knowledge of that information but did nothing with it is more likely to be a mercenary than a crook.
Having seen health plan price transparency data, I cannot unsee it. Considering its implications for the health economy has become almost all-consuming for me, a sentiment that the CEO and CFO of every U.S. company will eventually understand.
In fairness, seeing it requires processing it, and very few enterprises in the world understand the complexity of processing datasets that large, much less interpreting them. Health economy stakeholders love to talk about “big data,” and the health plan price transparency data is, to quote Buddy the Elf, “ginormous.” In fact, one month of machine-readable files from the “BUCHA” plans comprise over 100TB even when compressed, which is approximately 2/3 of the amount of data collected by the Hubble Telescope from 1990 to 2018.1
What do you see in these examples from health price transparency, and what would you do with it?
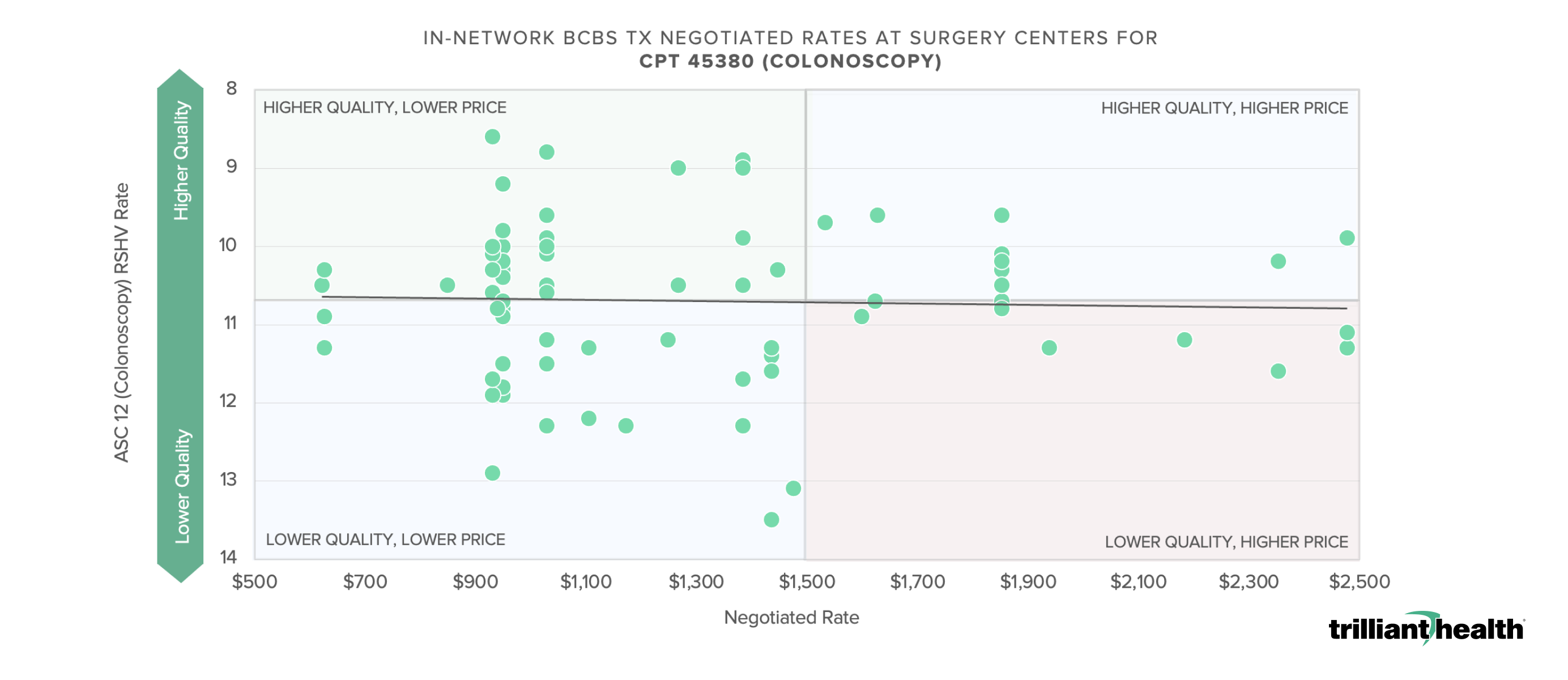
Note: Analysis was conducted using health plan price transparency Health Care Service Corporation negotiated rates (CMS definition) for surgery centers who billed code 45380 >250 times in 2022. (June 2023 file)
Source: Health Plan Price Transparency and Trilliant Health’s Provider Directory, and analysis of Ambulatory Surgical Center Quality Reporting (ASCQR) Program.

Note: Analysis was conducted using negotiated (CMS definition) for a single national payer. (June 2023 file)
Source: Health Plan Price Transparency and Trilliant Health's Provider Directory, and analysis of Hospital Readmissions Reduction Program (HRRP) data.
Perhaps more interesting than the people who haven’t seen the health plan price transparency data are those who don’t want to see it, primarily out of fear for what it reveals. Even so, the data indicts the entire industry, including:
- Carriers, for whom the intra-market variance in negotiated rates for the exact same service ranges from 2-6X throughout the U.S.;
- Health insurance brokers, particularly those who admit that they don’t want to know because it would impact their relationship with carriers;
- Policymakers focused on forcing hospitals to “do better” on hospital price transparency, apparently unaware that everything they want to codify is already contained in health plan price transparency data, other than the frequently cited but infrequently used cash price;
- Anyone and everyone who has promoted narrow networks, which depend on the fallacy that a small group of providers could deliver the highest value for all healthcare services in a market;
- Anyone and everyone who has promoted direct contracting, which compounds the fallacy of narrow networks by replacing scaled “administrative waste,” e.g., an ASO, with a different middleman with less scale;
- Companies and consultants suggesting that 100+ TB data can be queried accurately, and without limitations, in a timely manner in a user-friendly interface;
- Every health plan managed care executive responsible for negotiating premium rates for below-average quality, as well as every provider managed care executive responsible for negotiating below-market rates for above-average quality; and
- Anyone who requests that the exact amounts included in health plan price transparency files be converted into “percentage of Medicare” because it is “directionally correct” and “easier to understand.”
What does everyone indicted by health plan price transparency files have in common? Contentment with the status quo, the most daunting competitor of every health economy stakeholder. Why is the status quo no longer acceptable? Because the health plan price transparency files introduce new legal obligations for self-funded health plans, which we have previously highlighted.
In May, I wrote this:
As employers begin to discover how little value for money they are receiving – and specifically who the lowest value providers are – they may begin to think of “value-based care” as the British do: a reimbursement “scheme.” Employer CFOs will soon realize that health insurance brokers are mercenaries, not fiduciaries, even as those CFOs become increasingly aware of their fiduciary duty of care in the context of how employer healthcare costs impact net income.
In July, I wrote this:
In Delaware, directors and officers of corporations owe a fiduciary duty of care to the corporation and its stockholders, which requires them “to make informed business decisions” based on “the information that is material to the decision” and “to review the information critically.”2,3
Because health benefit costs are a material expense for every corporation that provides them, the advent of health plan price transparency implicates the fiduciary duty of care for directors and officers – especially chief financial officers – to “make informed business decisions” about health benefit costs using health plan price transparency data.
Since these posts, Kraft Heinz has sued Aetna for breach of fiduciary duty, law firms are reportedly seeking plaintiffs to represent against large plan sponsors, and last week the WSJ published an article about how employer coalitions – with the support of billionaire John Arnold, a former Enron trader – are trying to codify price caps.
Not surprisingly, the status quo has tried to block CMS’ Transparency in Coverage initiative, just as it did with HCAHPS and readmission penalties, and just as it is currently doing with prior authorization and interoperability. The status quo is healthcare’s version of Gollum’s Ring, the “my precious” subtly offering health economy stakeholders security and power:
On the whole, the Ring had a deleterious effect on mortals, although it prolonged their lives indefinitely. Such extension to their experience, however, added no value, as these mortals merely continued their existence in their formal states without any further development or growth. The Ring also captivated the mortals who wore it into an irresistible affinity and a reluctance to let go of it… Its greatest strength was its absolute control over all other forces.4 (Emphasis added)
Unlike Gollum’s Ring, which made the wearer invisible, the status quo is itself invisible, manifesting quietly in the form of lazy heuristics, reasoning by analogy and reliance on the “things we know” instead of facts.
Executive teams who fail to extinguish the status quo mindset in their organization sow the seeds of their own destruction, just as Gollum’s Ring did for everyone who clung to it. As General Eric Shinseki, the former Secretary of Veterans Affairs, famously said, “if you don’t like change, you’ll like irrelevance even less.”