























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Counterpoint
Hal Andrews | June 3, 2026The U.S. health economy is a major contributor to America’s approaching financial ruin. Knowing that motivates my quest to distinguish between the essential, the non-essential and the middleman grift, aka “administrative waste,” in the health economy.
The most frustrating aspect of the health economy’s copious middleman grift is the magnitude based on obviously flawed ideas. I have written previously about the sheer idiocy of the business model of cost-plus drugs, the enthusiasm for which is a startling testament to the apparent abstruse depths of grift in the pharmacy benefit management industry. However, one “innovative” idea is even more idiotic: “direct to employer contracting.”
Arnold Ventures-sponsored research makes this evidence-free declaration about direct to employer contracting:
“Direct contracting imposes downward pricing pressure and upward quality pressure to the health care market, eliminates administrative complexity, and alleviates provider burnout.”1
How is direct to employer contracting a salve for the woes of payer networks and third-party administrators (TPAs)?
“In direct contracting, providers commit to low payment rates for treatment bundles authorized by employers, freed from unpredictable revenue streams, administrative burdens, and resultant burnout. Since employers can steer their workers to direct contract providers, providers must compete on price and quality, therefore enabling market forces to drive efficiency towards quality and affordability. This dynamic creates a meaningful counterforce to consolidation in the provider market, benefiting employers and patients.
Historically, only TPAs have possessed the required technical infrastructure to administer such payments, making their involvement mandatory even in direct contracting arrangements and compromising the potential cost savings. Payer platforms are emerging to overcome this challenge, such as the partnership between Mishe Health and Mark Cuban's Cost Plus Wellness, which allows real-time adjudication, flexible benefit design, same-day provider payments, and transparent contract management.”2
Who knew it was so easy? All you need is to replace one set of middlemen – enterprise scale “one to many” models (UMR, Cigna, Meritain, Personify Health) – with a different and larger set of sub-scale middlemen. And “worker” steerage.
Oh.
Like the thought that any “cost-plus” model can reduce costs, the idiocy of direct to employer contracting as a salve for administrative waste is self-evident if one knows a few facts:
- According to the Bureau of Labor Statistics, 162.6M people were employed in the U.S. in April 2026.3
- According to the Census Bureau, in 2023 the U.S. had approximately 5.9M U.S. employer firms and 30.4M nonemployer businesses (sole proprietorships, independent contractors).4
- According to the Small Business and Entrepreneurship Council, only 0.3% of those employer firms had more than 500 employees, and only 1.9% had more than 100 employees.5
- According to the American Hospital Association, the U.S. has 5,127 community hospitals.6
The “California sober” thinking underpinning venture capital investment in direct to employer contracting models is evidenced by the fact that they are at best a “1% solution” to the very real problem of administrative waste.
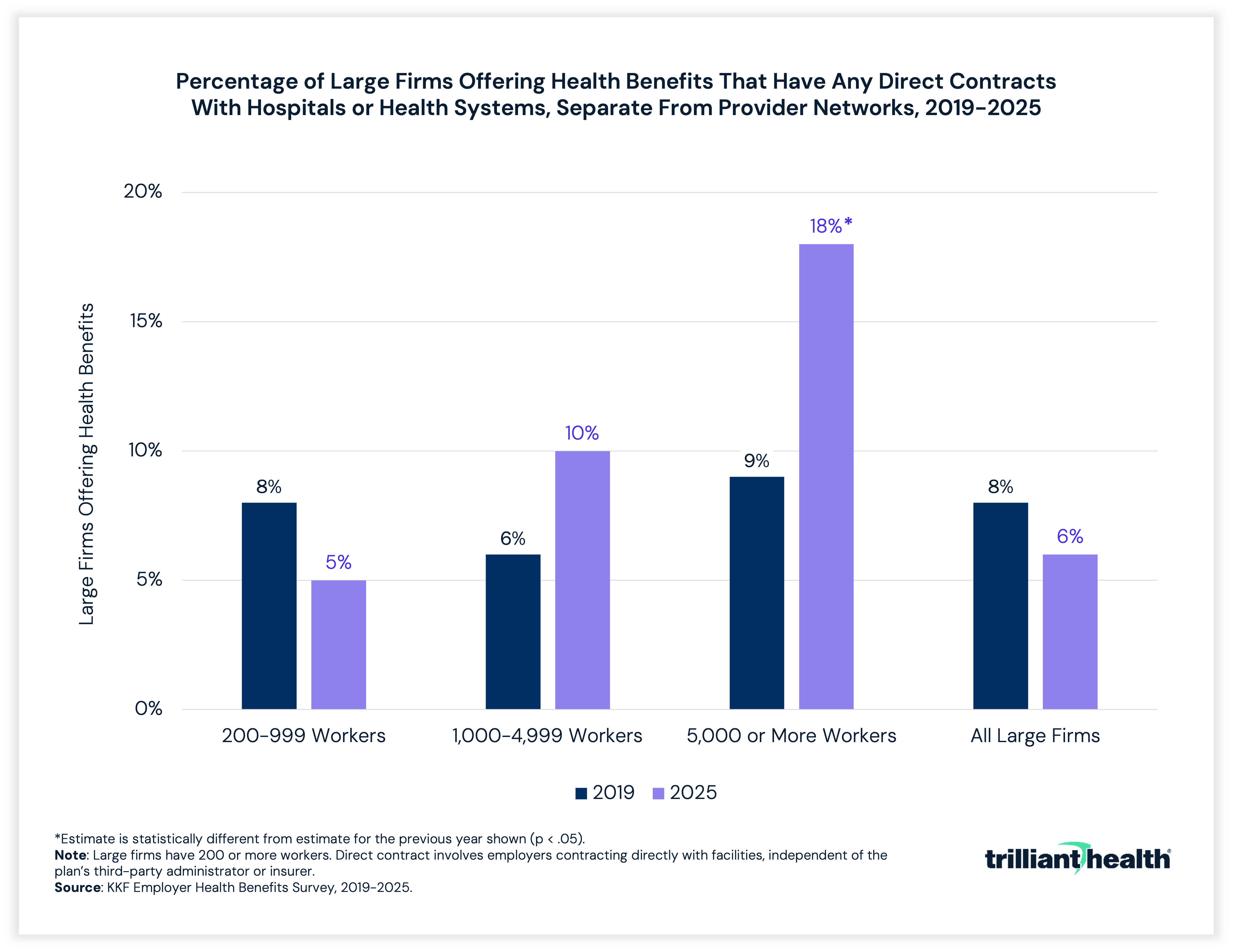
What the percentages in the above graph fail to reveal is that there were 2,262 employers with more than 5,000 employees in 2022, of which 546 firms employed 33.4M employees in aggregate.7 In theory, those employers have the scale to utilize direct to employer contracting. In reality, the ten largest employers with an aggregate of 7M employees – Walmart, Amazon, UPS, Home Depot, Target, Marriott, Kroger, UnitedHealth Group, Berkshire Hathaway and Starbucks – have the most distributed workforces in the country.8 In fact, six of those 10 employers operate in all 50 states and Puerto Rico, another in all 50 states, and another in 46 states, a scale that historically has required at least one national provider network.
Very simply, any direct to employer business model is an intermediary in an industry replete with them. The notion that a venture-capital-backed tech-enabled service can deliver value by effectively atomizing the scale of the incumbent TPAs is ludicrous, particularly those “innovative” models focused on specific service lines.
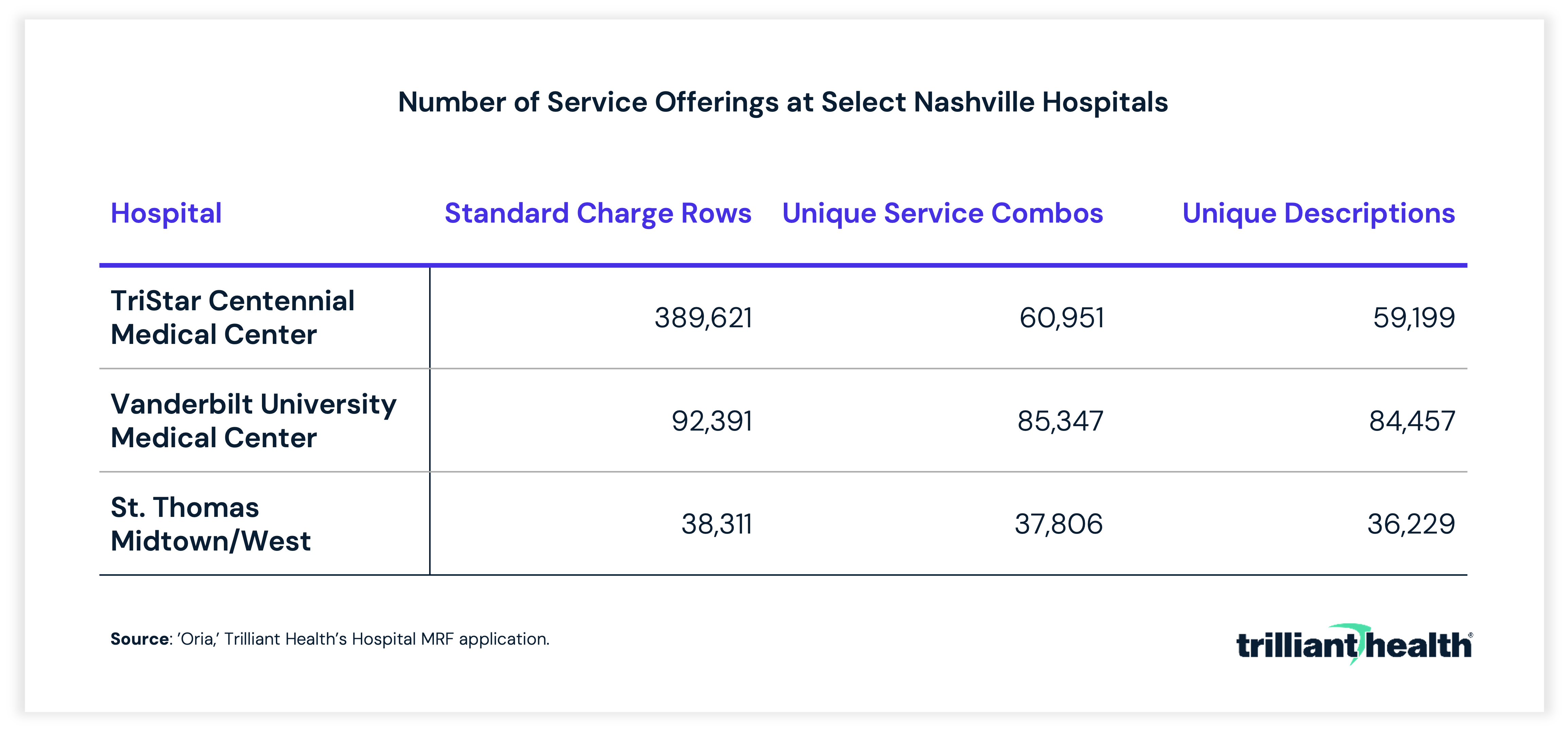
For example, our office is in a 400-acre business park with more than 600 businesses, hosting approximately 20,000 employees.9 For Ascension or HCA or Vanderbilt to contract directly with each of those businesses tailored to the needs of those 20,000 employees and their dependents is neither rational nor realistic given the complexity of their service offerings:
Given that many of the businesses in our office park have employees in multiple states, direct to employer contracting would require having direct to employer networks in multiple states to cover 100% of the workforce.
The First Law of Holes is axiomatic: if you find yourself in a hole, stop digging. Why would any rational person think that an approach that doesn’t produce meaningful results for even the Fortune 50 could work for the other 5.9M employer firms or 30.4M nonemployer businesses? And why would any rational and uninterested health economy stakeholder think that direct to employer contracting could reduce the administrative friction costs that currently exist? Reducing administrative waste in healthcare requires eliminating the existing middlemen, not disaggregating them.
Contrary to what the media and pundits and policymakers state, the problem with the U.S. healthcare system isn’t the “prices,” aka “charges,” which anyone who understands the first thing about the health economy knows are irrelevant. Similarly, the problem isn’t the lack of “price transparency,” i.e., commercially negotiated reimbursement rates, which I know in part since we have made all the hospital rates freely available.
Two things ail the health economy. One is the cost of delivering healthcare, which consists primarily of people and capital infrastructure, neither of which economic history suggests are easily susceptible to deflation. The other is that the variance in commercially negotiated reimbursement rates is nonsensical. More importantly, the rates do not represent fair market value.
The United States Department of Treasury (the “Treasury Department”) defines fair market value in accordance with the longstanding common law understanding of the term:
“The fair market value is the price at which the property would change hands between a willing buyer and a willing seller, neither being under any compulsion to buy or to sell and both having reasonable knowledge of relevant facts.”10
Notably absent from this definition is a mention of a broker or other intermediary. As a general principle, brokers of all kinds are intermediaries whose compensation introduces some level of compulsion for the buyer or the seller or both. From a fair market value perspective, the health economy is distorted by both commercial intermediaries – health insurance brokers and benefits consultants and group purchasing organizations and TPAs – and Federal and state regulatory and tax policies.
President Ronald Reagan described the government’s view of the economy this way:
“If it moves, tax it. If it keeps moving, regulate it. If it stops moving, subsidize it.”
President Reagan’s remark describes the truism that if you subsidize something, you get more of it.
Employer-sponsored health insurance is, of course, subsidized by the employer. What began, ironically, as a solution to wage inflation has spread to virtually every form of health insurance in the United States, most notably as a result of the Patient Protection and Affordable Care Act (PPACA), which was “designed” to make healthcare more “affordable” by subsidizing the cost of health insurance.
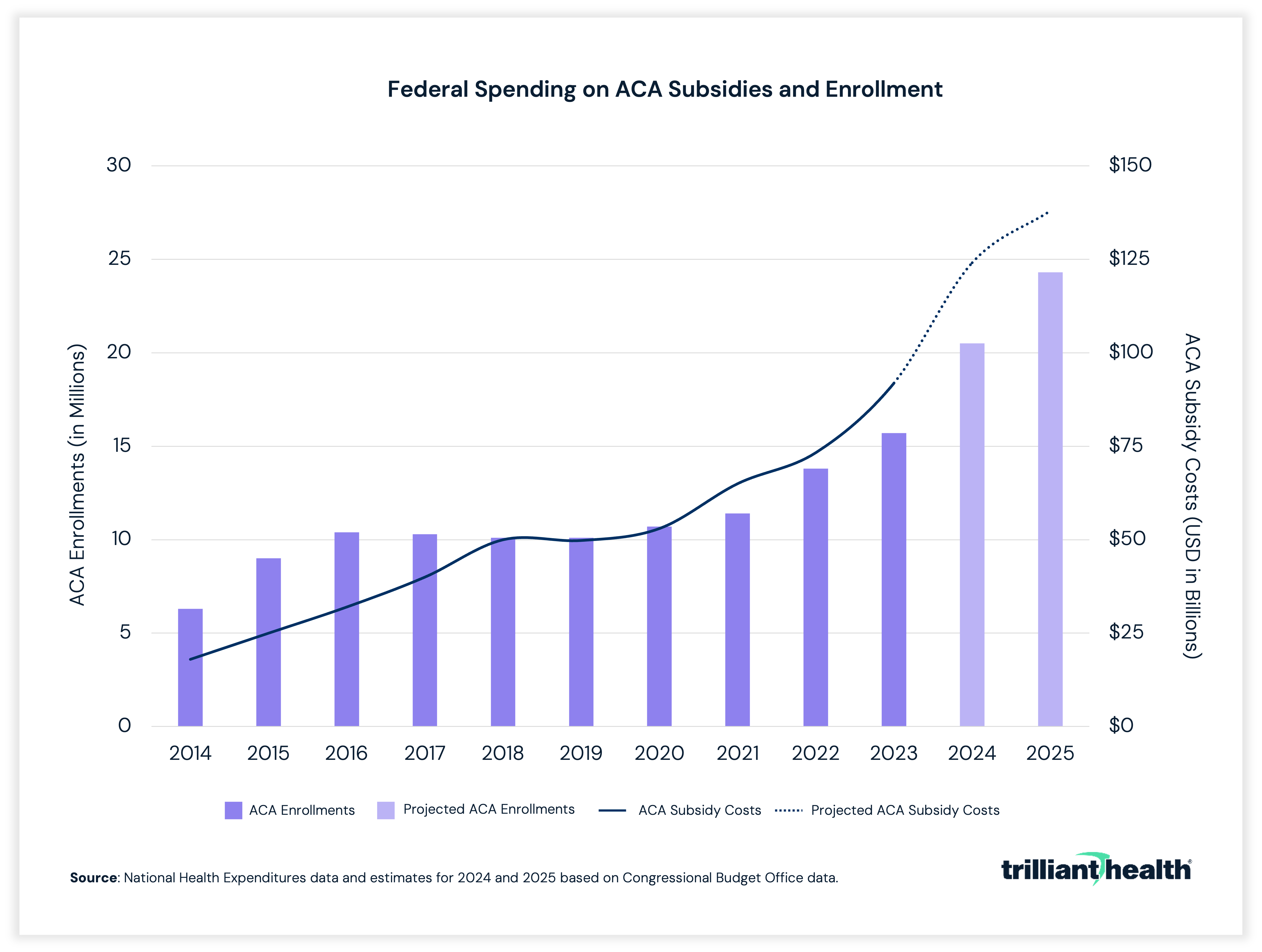
Since Congress made healthcare “more affordable” under the PPACA, U.S. healthcare GDP has increased from $2.5T in 2009 to $5.3T in 2024, an arc matched by another heavily subsidized sector, education.
In November 2023, I traced the history of employer-sponsored health insurance in a post surmising how Elon Musk might apply first principles thinking and what was then called the “Musk algorithm” to transform the U.S. healthcare system. On May 20, 2026, Musk’s Space Exploration Technologies Corp., aka SpaceX, filed a Form S-1 registration statement with the Securities and Exchange Commission (SEC).
If you are like me, you probably don’t think much about how to “ensure species-level redundancy” by colonizing Mars, but you might wonder how SpaceX designed a method to catch a rocket with “chopsticks” on its return to Earth. SpaceX credits its success to a business model “built on a repeatable, engineering-driven framework” executed through “core principles” that include “first-principles thinking” and application of “The Algorithm.”
“'The Algorithm' refers to our five-step iterative process that we use to rapidly innovate and optimize, emphasizing making the requirements less dumb, deleting unnecessary processes or parts, optimizing the necessary processes or parts, accelerating cycle timesteps, and automating only proven processes after the first four steps are completed.”11
In my November 2023 post, I wrote this:
“There is nothing that would unleash innovation in and transformation of the U.S. health economy more than the elimination of the tax deduction for employer-sponsored health insurance.”12
This idea is the unavoidable conclusion of first principles thinking about the health economy, as logically unassailable as it is politically unachievable. The fundamental question for you and every other health economy stakeholder is when the politically unachievable will become the politically unavoidable.
Until then, the unwillingness of Congress, employers and other health economy stakeholders to embrace the Occam’s razor solution leaves the harder work of applying “The Algorithm” to the macroeconomic issue of the rising cost of healthcare. It is immediately obvious that the dumbest aspect of the health economy is not merely the existence of the employer as the “buyer” of healthcare benefits for the majority of Americans but the massive tax incentives – which the Treasury Department projects at $296B for FY 2026 – that perpetuate the system.13 I keep waiting for employers to decide that the tax incentives are insufficient to compel their continued participation. Whether adoption of Individual Coverage Health Reimbursement Arrangement (ICHRA) plans becomes the “off-ramp” is, in my view, the most interesting signal in the health economy.
First principles thinking would ask these questions:
- Why does a provider have to be “in network”? What other industries require a seller to agree to a third party’s prices in advance to have the hypothetical right to meet a buyer? What are the cost trends in those industries?
- How are health insurance brokers necessary? Why are health insurance brokers paid via a commission? Why do Geico and Progressive advertise almost as much as pharmaceutical companies?
- What is a benefits consultant, and what tangible value do they deliver? Why aren’t their fees risk-based?
- Why are inpatient services and lab tests bundled but outpatient services are not?
- Why don’t providers offer volume discounts for services like physical therapy that will require multiple visits?
- Why aren’t encounters in the health economy paid for at the time of service, like groceries or gasoline or restaurants, or in advance, like airplane tickets or rent, resulting in a “receipt” instead of a “claim?”
- If a “claim” is necessary, why does it require “adjudication,” particularly by an unrelated third party?
- Why is the third party “adjudicator” allowed to generate income from holding the employer’s money while delaying the “remittance” to the service provider?
- Why do the most competitive markets, as defined by the Department of Justice and Federal Trade Commission, have the highest negotiated rates?
Utilizing “The Algorithm” would focus on the most efficient system to transfer a fair market value payment from the “purchaser” of healthcare services, i.e., the patient, to the “seller” of those services, i.e., the provider, as quickly as possible.
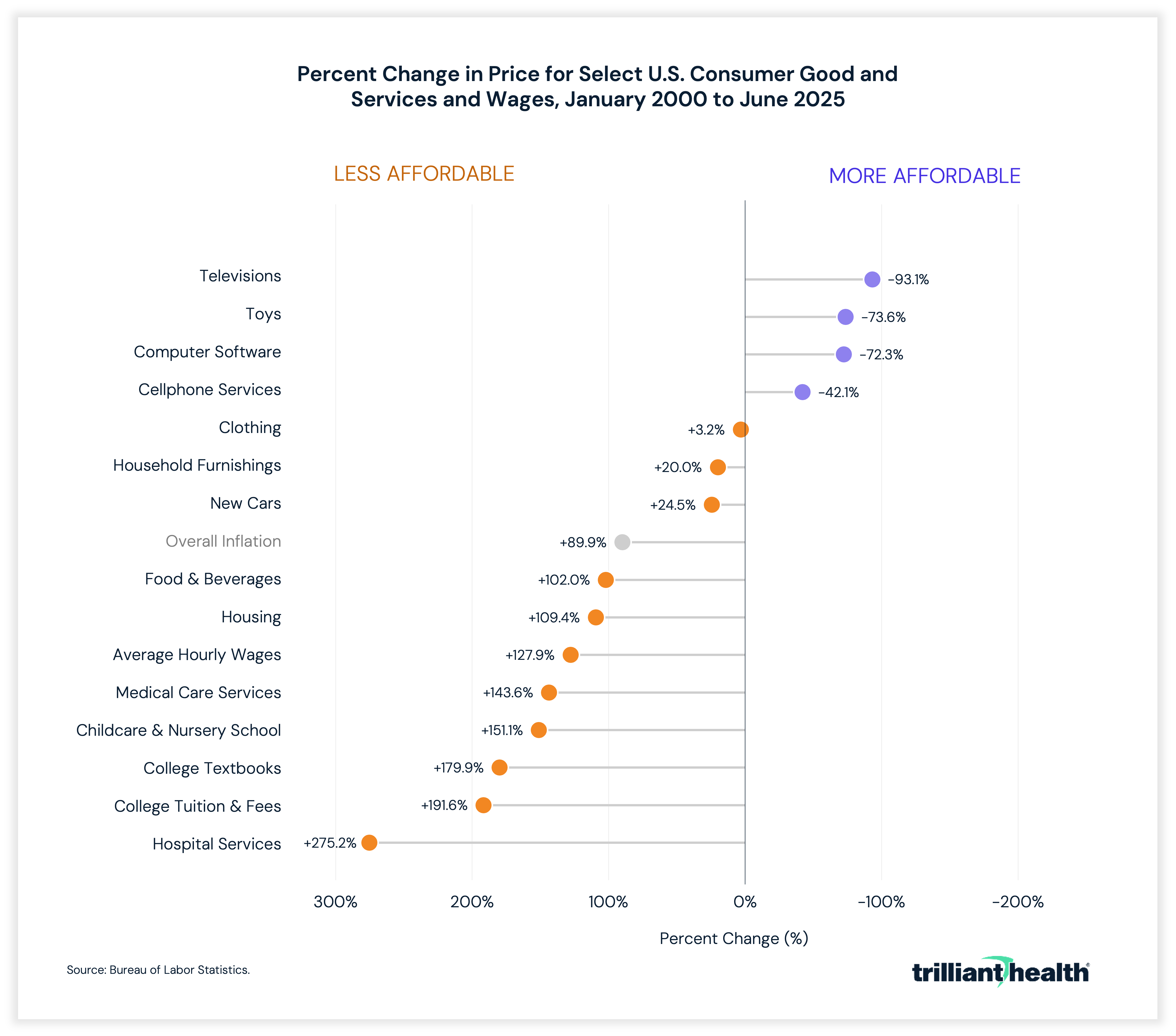
Cosmetic and LASIK surgery – which almost no employers subsidize as a “covered benefit” – offer examples of fair market value transactions in healthcare services. Perhaps unsurprisingly, the means and timing of value exchange in cosmetic and LASIK surgery mimic the rest of the economy – payment by cash or credit prior to or at the time of service. And, perhaps unsurprisingly and uncoincidentally given basic economic principles, the nominal cost of LASIK has increased only 10% since 2008.14
The inherent flaw in direct to employer contracting isn’t that it is effectively useless for 98% of employers but rather that it skips the first two steps of “The Algorithm” – “making the requirements less dumb, deleting unnecessary processes or parts” – while supposedly following the third - "optimizing the necessary processes or parts." Even so, viewed through the lens of first principles thinking, “The Algorithm” and the basic principles of economics, the core idea of direct to employer contracting is the foundation of an approach to reduce significant amounts of administrative complexity and waste in healthcare.
The economic law of demand is that, all things being equal, demand falls as prices rise, and vice versa. Included in the phrase “all things being equal” are all the middlemen in between a patient and a provider that obfuscate what fair market value is. Fair market value transactions are the lynchpin of any consumer-driven economy. For “healthcare consumerism” to work, “price transparency” is a prerequisite, but not a solution. And, as SpaceX has demonstrated, the real cost compression results from applying “The Algorithm” to understand the cost of the individual units of production, not the “price” of the finished good.
Employers that were truly motivated to reduce their health benefits cost and understood the necessity of fair market value transactions in healthcare would create a commercial insurance marketplace (the “Employer Healthcare Marketplace”) with the following characteristics:
- Instead of paying TPAs for network access, the Employer Healthcare Marketplace would be an “any willing provider” network. Any and every provider – hospitals, ambulatory surgery centers, physician groups, etc. – could post the reimbursement rates – in cash prices – at which they would deliver a defined set of services to any commercially insured individual. As a condition of participation in the Employer Healthcare Marketplace, each provider would be required to post electronic links for physician or clinic visit scheduling.
- Instead of paying TPAs for “claims adjudication,” the Employer Healthcare Marketplace could leverage blockchain technology to act as an escrow service, which would enable an employer or employee to pay the agreed upon price upon documentation of receipt of care.
- The Employer Healthcare Marketplace would then utilize the distributed ledger of that blockchain as a source of activity for relevant government-mandated quality measures, as well as a frequently asked questions section to include information like recommendations from the United States Preventive Services Task Force.
In today’s world, the technical challenges of creating an Employer Healthcare Marketplace are straightforward. The issue, as always with employers, is the will to slay the status quo.
Why the 5.9M employer firms are not doing more to control their expenditures on employee healthcare benefits is puzzling, recalling Walt Kelly’s Pogo: “We have met the enemy, and he is us.” Even if no employer wants to manage healthcare benefits, every employer has fiduciary duties not to waste their resources. Based on healthcare cost trends, why employers continue to seek solutions from their benefits consultants and brokers recalls the definition of insanity.
Health economy stakeholders are seemingly unaware that cost controls are imminent, whether mandated by Federal and state governments through price controls or catalyzed by employers through a demand for value for money. If providers and life sciences companies understood the magnitude of existing and forthcoming government price caps, they would be begging employers to establish an exchange similar to what is described above.
As for the grifters, remember this: pigs get fat, and hogs get slaughtered.