























.png)

















.png?width=171&height=239&name=2025%20Trends%20Report%20Nav%20(1).png)

Counterpoint
Hal Andrews | July 1, 2026Note: This post is an updated and revised version of a post that appeared in two parts on July 7, 2017 and July 11, 2017.
Almost 250 years ago, the Founding Fathers wrote these words:
“When in the Course of human events it becomes necessary for one people to dissolve the political bands which have connected them with another and to assume among the powers of the earth, the separate and equal station to which the Laws of Nature and of Nature's God entitle them, a decent respect to the opinions of mankind requires that they should declare the causes which impel them to the separation.
We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness. — That to secure these rights, Governments are instituted among Men, deriving their just powers from the consent of the governed, — That whenever any Form of Government becomes destructive of these ends, it is the Right of the People to alter or to abolish it, and to institute new Government, laying its foundation on such principles and organizing its powers in such form, as to them shall seem most likely to effect their Safety and Happiness.”1
Almost 143 years ago, the poet Emma Lazarus wrote these words that are on a bronze plaque next to the Statue of Liberty:
“Give me your tired, your poor,
Your huddled masses yearning to breathe free,
The wretched refuse of your teeming shore.
Send these, the homeless, tempest-tossed to me,
I lift my lamp beside the golden door!”2
U.S. Healthcare Policy Through the Lens of America’s Founding Principles
Viewed through the prism of these words, the paucity of thoughtful healthcare policy in Washington, D.C. and various state legislatures is distressing to witness and embarrassing to this great country. Democrats and Republicans should be ashamed of the cowardly and cynical way in which they have addressed healthcare policy for decades.
In 2006, I approached the campaigns of then Representative Harold Ford, Jr. and then Senate candidate Bob Corker with a proposal for a healthcare plan with these elements:
- Establishment of a health savings account (HSA) for every child born in America linked to their Social Security number;
- Government funding of $2,000 per year into every child’s HSA until the child turned 18;
- Government-sponsored insurance policy for each child for any catastrophic medical conditions or disease that developed in childhood; and
- Between the ages of 18 and 22, allow the beneficiary to keep the HSA or convert the balance into an account tied to a 529 plan.
Representatives of each campaign politely listened and then suggested that I would have the most impact by writing a check to their campaign.
In 2010, the Patient Protection and Affordable Care Act, aka the ACA, became the law of the land. The ACA, which I have read in its entirety, is terrible legislation in so many ways, as would be expected of a 900-page behemoth that contains the phrase “the Secretary shall” 1,442 times and was largely crafted by a group whose exposure to life outside the Beltway is attending the Virginia Gold Cup. Something that affects almost 20% of the economy and 100% of Americans should have been based on a “Great Compromise” derived from an open conversation with the American people, not naked political opportunism by 279 people with a limited understanding of healthcare policy and delivery.
Despite being modeled on certain aspects of England’s National Health Service (NHS), the public perception of the ACA is distinctly different than that of the NHS, which, despite its well-documented problems, is a source of pride to the British.3 The reason? The British actually thought about whether access to healthcare services was a privilege or a fundamental right, highlighted by the 1942 Beveridge Report that led to the creation of the NHS in 1948.
Notably, the NHS has a constitution that includes its seven foundational principles:
- “The NHS provides a comprehensive service, available to all.
- Access to NHS services is based on clinical need, not an individual’s ability to pay.
- The NHS aspires to the highest standards of excellence and professionalism.
- The patient will be at the heart of everything the NHS does.
- The NHS works across organizational boundaries.
- The NHS is committed to providing best value for taxpayers’ money.
- The NHS is accountable to the public, communities and patients that it serves.”4
Unfortunately for Americans, our politicians either don’t care what we think or believe they know better or are unconcerned about a national conversation about the philosophical underpinnings of an industry that commands 18% of the U.S. GDP and 4.8% of global GDP.5,6
What the Founding Fathers Might Think
Nature abhors a vacuum, so the absence of a meaningful national dialogue prompts me to evaluate my now 19-year-old proposal against America’s two foundational legal documents. Applying first principles thinking, of which I am fond, to the words of the Founding Fathers leads me to several initial conclusions.
First, given the inability or unwillingness of our elected officials to collaborate and act constructively, I believe that Americans are entitled to “dissolve the political bands,” whether figuratively by sharing their thoughts through letters, emails and town halls or practically by sending an entirely new team to Washington. I expect the latter to manifest on November 7, 2028.
Second, out of “a decent respect to the opinions of mankind,” I believe Americans “should declare the causes which impel them to the separation” of the politicians from their offices by insisting that American citizens should have the controlling voice in the discussion about whether healthcare is a privilege or an “unalienable Right.”
Third, holding “these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness,” the cornerstone of any national healthcare policy would seemingly be that every citizen – whether poor or rich or terminally ill or vibrantly healthy – would be treated equally. Logically, only a policy that applies to Americans based on equivalent status (e.g., poverty level) or objective fact (e.g., birth or age) can be truly equal. Today, Traditional Medicare is the only U.S. healthcare policy that meets that standard.
Fourth, and most compelling from a policy standpoint, providing a financial foundation from birth should reduce inequalities in health and healthcare access across gender, ethnicity, location and any other category, as every child would have the same resources to pay for their care. With readily available and accessible primary care for citizens for the first 18 years of their life, health status should improve and healthcare costs should decline. Furthermore, this approach could lead to a cultural shift in how individuals perceive and interact with their own health and healthcare, leading to long-term improvements.
Such a result would “seem most likely to effect their Safety and Happiness.” And it would certainly enable America to serve its “tired…poor…huddled masses yearning to breathe free” more equitably and efficiently.
While it is easy to believe that the Founding Fathers would not object conceptually to a plan that treats all natural-born citizens equally from birth, it is difficult to believe that the Founding Fathers would have envisioned the implementation of Medicare, Medicaid or Social Security. It is certain that Alexander Hamilton would be appalled at the 2026 Medicare Trustees Report, but most policymakers are more enamored of Lin-Manuel Miranda’s Hamilton than the first Secretary of the Treasury. The latter wrote this of himself in the third person:
“...that he ardently wishes to see it incorporated, as a fundamental maxim in the system of public credit of the United States, that the creation of debt should always be accompanied with the means of extinguishment. This he regards as the true secret for rendering public credit immortal.
...
The debt too may be swelled to such a size, as that the greatest part of it may cease to be useful as a capital, serving only to pamper the dissipation of idle and dissolute individuals; as that the sums required to pay the interest upon it may become oppressive, and beyond the means which a government can employ, consistently with its tranquility, to raise them; as that the resources of taxation, to face the debt, may have been strained too far to admit of extensions adequate to exigencies, which regard the public safety.”7
(Emphasis added)
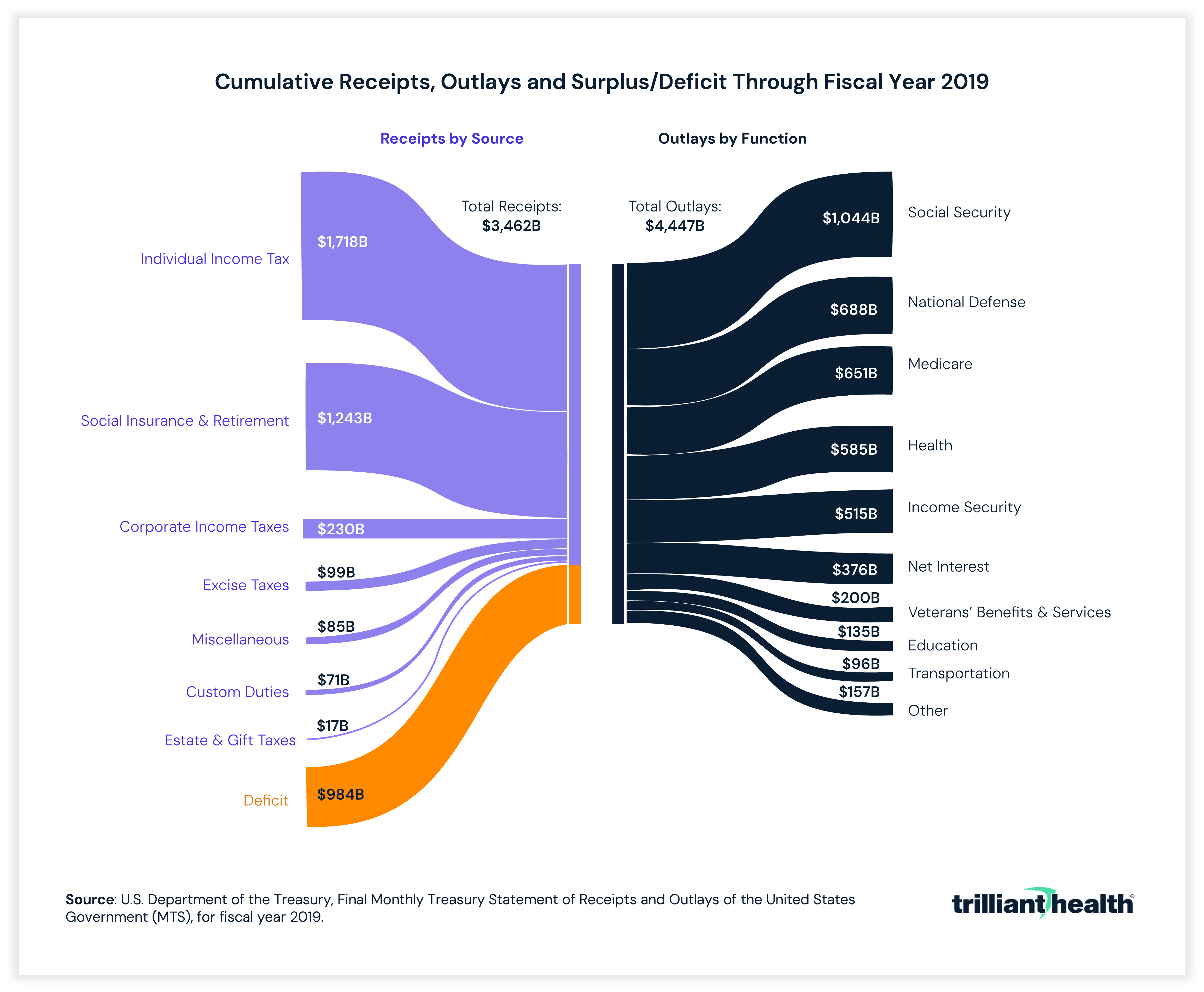
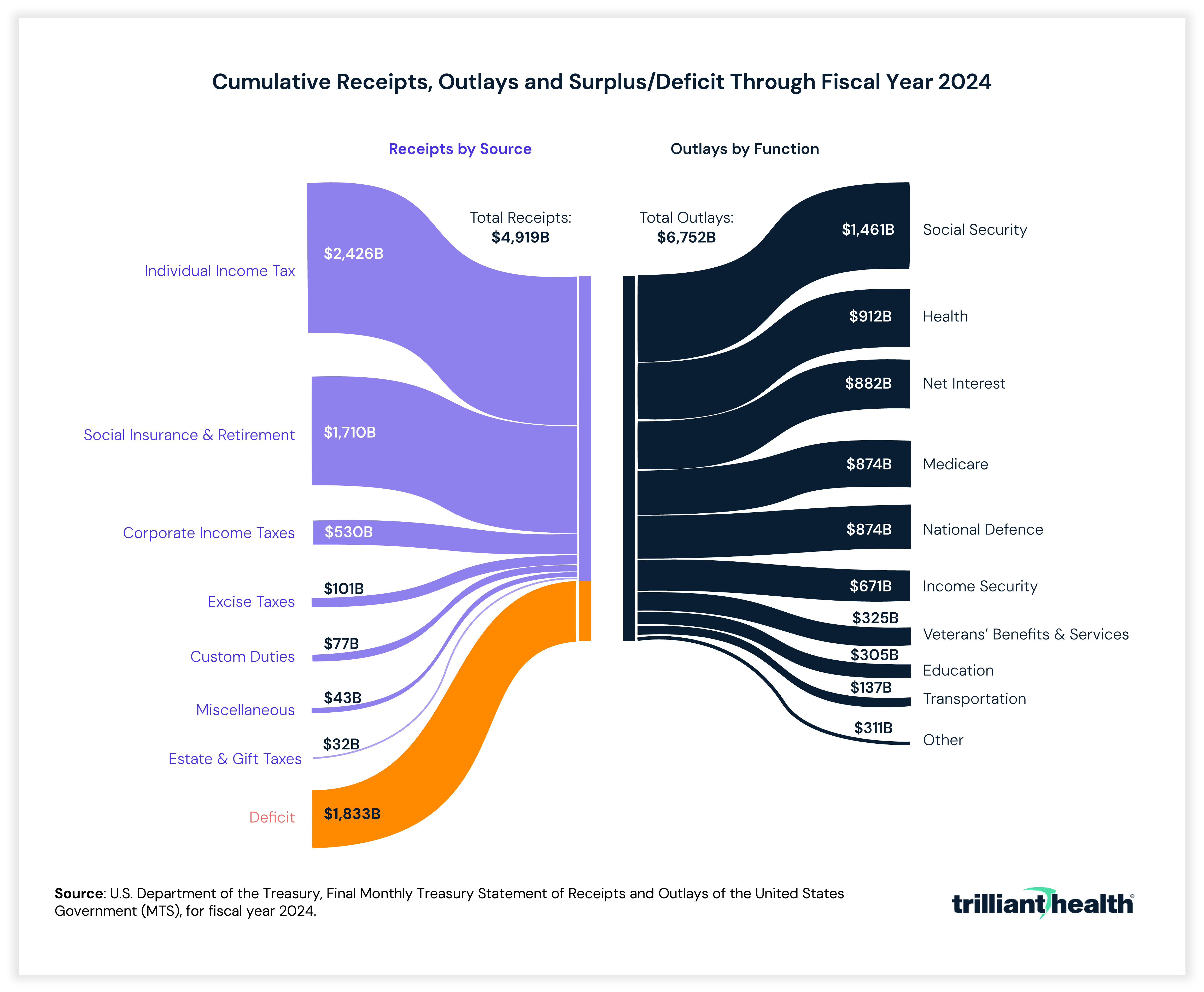
Based on those statements, Hamilton – and Jefferson, Franklin and others – would be distressed by this trend:
FMAP: The Constitutional and Fiscal Problem
The Constitution and the Bill of Rights are, unsurprisingly, silent about a national healthcare system. Article I, Section 8 of the Constitution, aka the “Spending Clause,” states that “Congress shall have Power To lay and collect Taxes, Duties, Imposts and Excises, to pay the Debts and provide for the common Defence and general Welfare of the United States; but all Duties, Imposts and Excises shall be uniform throughout the United States.”8 However, “No Money shall be drawn from the Treasury, but in Consequence of Appropriations made by Law.”9 Under the Tenth Amendment, “powers not delegated to the United States by the Constitution, nor prohibited by it to the States, are reserved to the States respectively, or to the people.”10
While a “strict constructionist” might deny the legitimacy of a national healthcare system under the Tenth Amendment, most legal scholars would approve of such a system based upon the allowance of “Bills for raising Revenue” in Article I, Section 7 and the Spending Clause of Article I, Section 8.11 However, the language of Article I, Section 8 implicitly requires such a program to be funded fully with tax dollars, which the Founding Fathers would certainly require based upon a review of their correspondence and the Federalist Papers.
Implicit in Congress’ fiscal power is the responsibility to exercise it prudently, as summarized by President Thomas Jefferson:
“It is a wise rule, and should be fundamental in a government disposed to cherish it’s [sic] credit, and at the same time to restrain the use of it within the limits of it’s [sic] faculties, ‘never to borrow a dollar without laying a tax in the same instant for paying the interest annually, and the principal within a given term: and to consider that tax as pledged to the creditors on the public faith.”12
From a purely Constitutional view, Medicare and Social Security are funded primarily through payroll taxes, which Congress explicitly has the “power to lay and collect.” Moreover, there is a clear, if partial, nexus between an individual “paying into” Medicare and Social Security prior to receiving benefits from those programs. As such, neither Medicare nor Social Security merits constitutional scrutiny.
Medicaid, however, is distinctly different from Medicare and Social Security because it is funded jointly by the Federal government and the states. Under the Spending Clause, Medicaid would not merit any constitutional scrutiny if it were fully funded by Congress through “block grants” or on a per capita basis or, alternatively, left to the discretion of the individual states per the Tenth Amendment. However, the Founding Fathers might believe that the current funding of Medicaid is unconstitutional.
Congress describes Medicaid funding this way:
“Medicaid is a means-tested entitlement program that finances the delivery of primary and acute medical services as well as long-term services and supports. Medicaid is jointly funded by the federal government and the states. The federal government's share of most Medicaid expenditures is called the Federal Medical Assistance Percentage (FMAP). The remainder is referred to as the state share…
Generally determined annually, the FMAP formula is designed so that the federal government pays a larger portion of Medicaid costs in states with lower per capita incomes relative to the national average (and vice versa for states with higher per capita incomes). FMAP rates have a statutory minimum of 50% and a statutory maximum of 83%. For FY2025, regular FMAP rates range from 50.00% (10 states) to 76.9% (Mississippi).
The FMAP rate is used to reimburse states for the federal share of most Medicaid expenditures…
While many FMAP exceptions are used to incentivize states, the FMAP rate also can be used as a means to penalize states through a reduction to the FMAP rate.”13
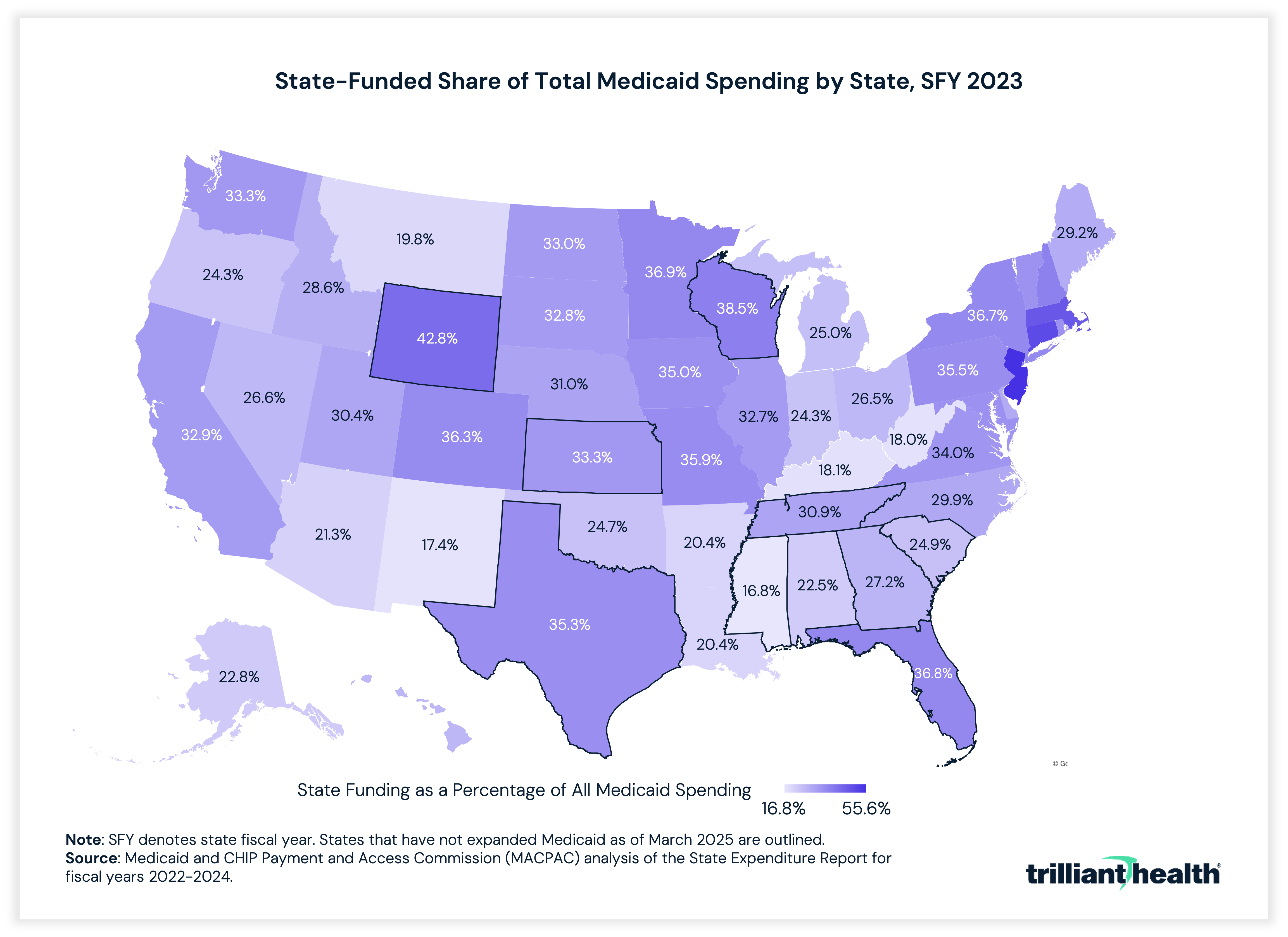
As a result, Medicaid is both a revenue source for state governments, i.e., the Federal matching funds, and an expense. Some states receive as much as $4 in “federal matching funds” for every $1 the state spends, as the following graph depicts:
In 2017, Forbes detailed the perverse incentives that FMAP creates:
“Medicaid financing essentially is a self-inflicted ‘tragedy of the commons’[1]… Just as the ‘commons’ encourages rational farmers to keep adding more sheep to the commons because they have failed to consider the adverse impact of their actions on other farmers, the FMAP encourages every state to increase Medicaid spending more than it would otherwise. Every state has to balance its spending on Medicaid against its spending on K-12 education, higher education, transportation, corrections, public assistance and other priorities. Such decisions are greatly distorted when states know they can receive $1 to $3 from Uncle Sam for every state dollar put into Medicaid. The enhanced match rate distorts things drastically greater by giving them 9 federal dollars for every state dollar used for the expansion.”14
That the political class and national media know, but obfuscate, the reality of FMAP while clamoring about Medicaid “cuts” is maddening. Serious people are not discussing “cutting” Medicaid spending but rather slowing its projected future rate of growth. In fact, Medicaid spending has declined only once in 60 years – can you spot it?
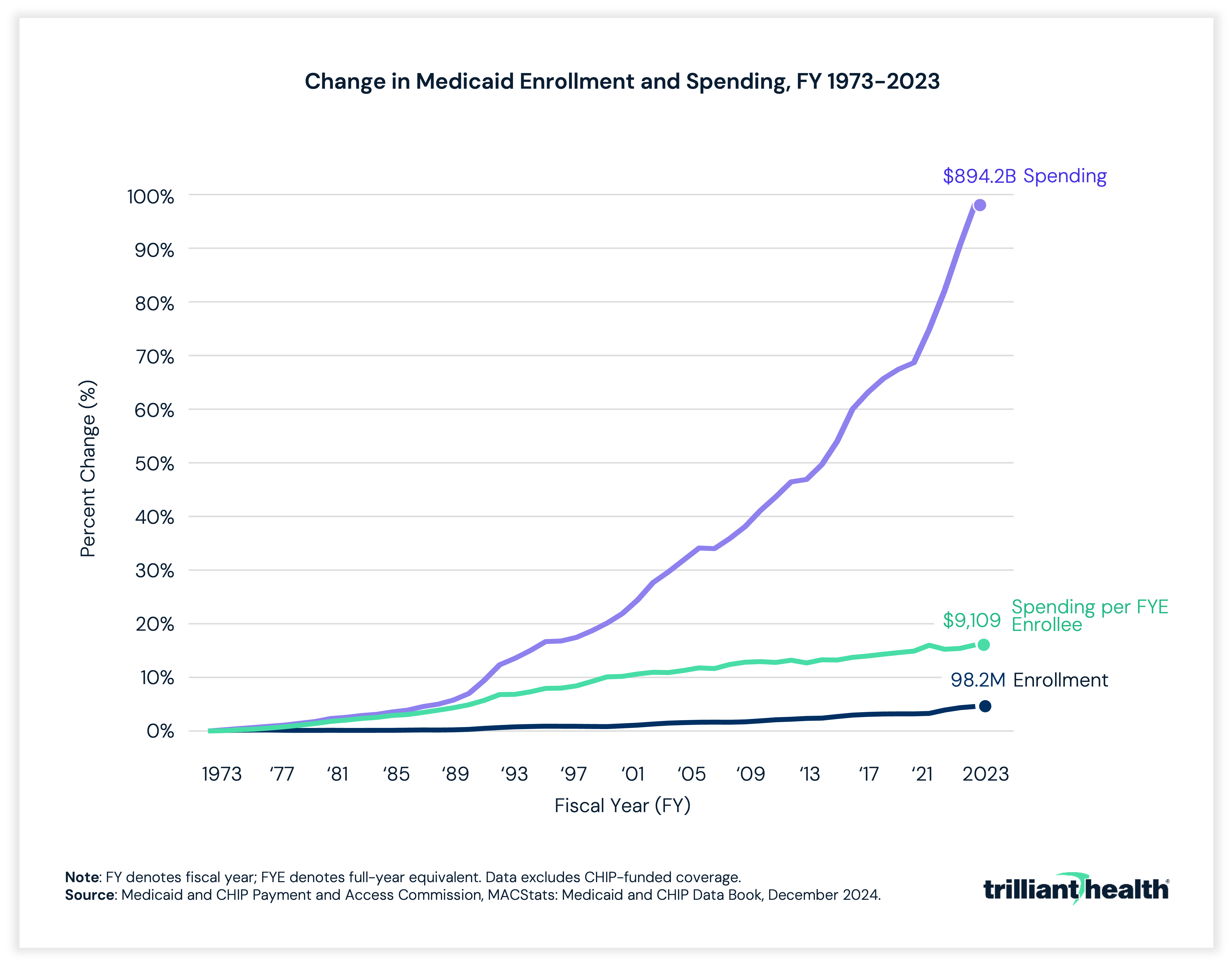
The explosive growth in Medicaid – from $0 to $1,000,000,000,000 – in 60 years means that America spends more per capita on Medicaid than any other country spends on their entire population. A critical question facing America is how fast Medicaid will grow, and at what cost to other initiatives.
It is difficult to imagine a Federal policy more discriminatory against America’s most vulnerable citizens or more threatening to America’s fiscal health than FMAP. Even if FMAP does not present a constitutional problem for Americans, it seemingly presents an existential one.
The Difference Between Good Intentions and Effective Policy
Medicaid was originally designed for poor women, their dependent children and the disabled. Because the Founding Fathers undoubtedly knew that some people “created equal” and “endowed by their Creator with certain unalienable Rights” end up disadvantaged with respect to economic, physical and mental health, they would likely think that the legislative intent of Medicaid was laudable.
Hamilton presciently wrote in the Federalist Papers: No. 33:
“The Convention probably foresaw, what it has been a principal aim of these papers to inculcate, that the danger which most threatens our political welfare is that the State governments will finally sap the foundations of the Union;”15
Whether Medicaid policy is the manifestation of Hamilton’s fear that “State governments will finally sap the foundations of the Union” is a question for every health economy stakeholder, and probably every American. Medicaid is a prime example of the notion that if you subsidize something, you get more of it. The political brilliance of Medicaid is that it is unmatched in scale as a bribe from the Federal government to the states, which is the reason no state Attorney General has ever challenged its constitutionality.
The Supreme Court did, in a 5-4 decision, famously uphold the constitutionality of Medicaid expansion under the ACA in National Federation of Independent Business v. Sebelius, aka the “individual mandate” case.16 Implicit in Chief Justice Roberts’ opinion was that the Medicaid program is a valid exercise of the Spending Clause:
“Congress may also ‘lay and collect Taxes, Duties, Imposts and Excises, to pay the Debts and provide for the common Defence and general Welfare of the United States.’ U. S. Const., Art. I, § 8, cl. 1. Put simply, Congress may tax and spend. This grant gives the Federal Government considerable influence even in areas where it cannot directly regulate…And in exercising its spending power, Congress may offer funds to the States, and may condition those offers on compliance with specified conditions. See, e. g., College Savings Bank v. Florida Prepaid Postsecondary Ed. Expense Bd., 527 U. S. 666, 686 (1999). These offers may well induce the States to adopt policies that the Federal Government itself could not impose. See, e. g., South Dakota v. Dole, 483 U. S. 203, 205– 206 (1987) (conditioning federal highway funds on States raising their drinking age to 21).”17
More generally, Chief Justice Roberts’ opinion rests upon the presumption that Medicaid is a valid exercise of Congress’ enumerated powers:
“The second provision of the Affordable Care Act directly challenged here is the Medicaid expansion. Enacted in 1965, Medicaid offers federal funding to States to assist pregnant women, children, needy families, the blind, the elderly, and the disabled in obtaining medical care. See 42 U. S. C. § 1396a(a)(10). In order to receive that funding, States must comply with federal criteria governing matters such as who receives care and what services are provided at what cost. By 1982 every State had chosen to participate in Medicaid. Federal funds received through the Medicaid program have become a substantial part of state budgets, now constituting over 10 percent of most States’ total revenue.”18
From a purely legal standpoint, it is curious why the dozens of Attorneys General and other attorneys involved in the case argued that Medicaid expansion was unconstitutional without challenging the constitutionality of Medicaid itself. Indeed, Chief Justice Roberts’ opinion seems to invite that argument:
“The Commerce Clause is not a general license to regulate an individual from cradle to grave, simply because he will predictably engage in particular transactions. Any police power to regulate individuals as such, as opposed to their activities, remains vested in the States.”19
In his opinion, Chief Justice Roberts cites this well-established legal principle:
“Such laws, which are not ‘consist[ent] with the letter and spirit of the constitution,’ McCulloch, supra, at 421, are not ‘proper [means] for carrying into Execution’ Congress’s enumerated powers. Rather, they are, ‘in the words of The Federalist, ‘merely acts of usurpation’ which ‘deserve to be treated as such.’ Printz v. United States, 521 U. S. 898, 924 (1997) (quoting The Federalist No. 33, at 204 (A. Hamilton); alteration omitted); see also New York, 505 U. S., at 177; Comstock, supra, at 153 (Kennedy, J., concurring in judgment) (‘It is of fundamental importance to consider whether essential attributes of state sovereignty are compromised by the assertion of federal power under the Necessary and Proper Clause . . . ‘).”20
Later, Chief Justice Roberts cites another well-established legal principle:
“We have long recognized that Congress may use this power to grant federal funds to the States, and may condition such a grant upon the States’ ‘taking certain actions that Congress could not require them to take.’ College Savings Bank, 527 U. S., at 686…At the same time, our cases have recognized limits on Congress’s power under the Spending Clause to secure state compliance with federal objectives. ‘We have repeatedly characterized . . . Spending Clause legislation as ‘much in the nature of a contract.' Barnes v. Gorman, 536 U. S. 181, 186 (2002) (quoting Pennhurst State School and Hospital v. Halderman, 451 U. S. 1, 17 (1981)). The legitimacy of Congress’s exercise of the spending power ‘thus rests on whether the State voluntarily and knowingly accepts the terms of the ‘contract.’”21
Together, these two well-established principles allow Congress to incentivize states to do things that Congress cannot compel the states to do so long as those actions are “consistent with the letter and spirit of” the Constitution.
The Tenth Amendment would explicitly allow each state to design and fund a program to provide health insurance benefits to some or all its residents, or not to do so, since providing health insurance benefits is not an enumerated power of Congress. Similarly, under the Spending Clause, Congress could undoubtedly authorize the Federal government to underwrite health insurance benefits for low-income Americans as it has for elderly Americans under Medicare. In dissent, Justice Ginsburg concurs:
“In 1965, Congress elected to nationalize health coverage for seniors through Medicare. It could similarly have established Medicaid as an exclusively federal program. Instead, Congress gave the States the opportunity to partner in the program’s administration and development. Absent from the nationalized model, of course, is the state-level policy discretion and experimentation that is Medicaid’s hallmark; undoubtedly the interests of federalism are better served when States retain a meaningful role in the implementation of a program of such importance.”22
Even if the states have the discretion to accept Federal funding to undertake “certain actions that Congress could not require them to take,” those actions must not violate the Constitution, as the Supreme Court ruled in South Dakota v. Dole:
“Instead, we think that the language in our earlier opinions stands for the unexceptionable proposition that the power may not be used to induce the States to engage in activities that would themselves be unconstitutional.”23
As such, it is unclear why the Federal government is permitted not only to endorse but through FMAP explicitly to incentivize unequal treatment of low-income Americans within and among the states with respect to Medicaid benefits. How can the Federal government underwrite a smaller benefit for a resident who is disabled and poor than for a resident who is able-bodied and poor? Such an outcome is at least antithetical to the spirit of the Declaration of Independence, if not the express provision of the Fourteenth Amendment guaranteeing “the equal protection of the laws.” Curiously, Justice Ginsburg extols that very fact:
“Subject to its basic requirements, the Medicaid Act empowers States to ‘select dramatically different levels of funding and coverage, alter and experiment with different financing and delivery modes, and opt to cover (or not to cover) a range of particular procedures and therapies. States have leveraged this policy discretion to generate a myriad of dramatically different Medicaid programs over the past several decades.’ Ruger, Of Icebergs and Glaciers, 75 Law & Contemp. Prob. 215, 233 (2012) (footnote omitted).”24
Whether Medicaid survives Constitutional scrutiny, there is nothing more inequitable in healthcare than Medicaid, which differentiates among low-income Americans based on the state of their residence.
What the Founding Fathers Might Build
Imagine, if you will, that the Supreme Court ruled that Medicaid, as currently implemented, violates some combination of the Tenth and Fourteenth Amendments. What should or would Congress do? How might the Founding Fathers approach the idea of a national healthcare plan that embodied the ideals of the Declaration of Independence and constitutional principles?
First, there is no evidence that the Founding Fathers would think that free healthcare is an “unalienable Right.” Second, the Founding Fathers’ foundational ideal of equality, while desperately flawed in execution with respect to slavery, would suggest equal treatment of those benefitting from a national healthcare plan, whether all or a subset of citizens. Third, Article I, Section 9’s prohibition on any capitation or direct tax disproportionate to the Census suggests that the Founding Fathers would have expected that Federal appropriations for a national healthcare plan be apportioned on a per capita basis. Fourth, it is certain that at least Benjamin Franklin would insist upon work requirements of some sort – and maybe even temperance – to be eligible to participate in a national healthcare plan. Fifth, and most importantly, in 2026, the Founding Fathers would analyze the proposed scope of a national healthcare plan in terms of what America can afford.
The intentional flexibility of the Constitution allows for numerous approaches to a national healthcare plan for America’s most vulnerable citizens consistent with those principles. Perhaps unsurprisingly, my 2006 proposal is harmonious with the Declaration of Independence and the Constitution, treating every child “born…in the United States,” in the language of the Fourteenth Amendment, equally.
Consistent with the original intent of Medicaid, it would also clearly be constitutional for the Federal government to provide pre- and post-natal healthcare benefits for every expectant mother, with coverage retroactive to the first day of the first gestational month and continuing for some pre-defined post-natal period. Notably, underwriting a benefit to cover all pregnancies would be straightforward, as would reinsuring against pre-term births, birth traumas (e.g., abruptions) and other catastrophic outcomes.
Similarly, the Federal government could lawfully provide lifetime health insurance coverage for every permanently disabled citizen or establish a plan that provided equal benefits to every American citizen based on objective measure, e.g., a percentage of Federal Poverty Level. More broadly, President Harry Truman’s desire for universal healthcare coverage, which today is described as “Medicare for All,” would clearly be constitutional if funded solely by the Federal government.
Whether Medicaid, as currently implemented, complies with the Constitution is a question that should have been asked long ago of the Supreme Court. It is ironic that a program designed for the poor and disabled has become so enormous that the political class is constitutionally incapable of doing right by the poor and disabled. The greed that reveals itself in the “policymaking” for national defense is unseemly enough; to see that behavior around a program for the poor and disabled is abhorrent.
Even so, the Founding Fathers would likely be astonished that a country that was practically insolvent at inception could have created a health insurance program that covers fewer than 1% of the global population at a cost of $1 out of every $100 of global GDP and yet treats beneficiaries unequally. A reasonable person would think that for $1T per year – or even less – America could equitably provide excellent healthcare for our tired and poor and huddled masses, our disabled and our expectant mothers and our children.
With their familiarity with English law, the Founding Fathers would likely question whether Americans receive the “best value for taxpayers’ money” for Medicaid, which might prompt other questions:
- Does America have the resources to care for children and the physically and mentally disabled? Of course.
- Does the current financing of those resources through Medicaid create perverse incentives for behavior that is not solely focused on caring for children and the poor and the disabled? Absolutely.
- Would a Tenth Amendment approach lead to a more unequal system? Without question.
- Does anyone in Washington, D.C. realize that the intensity of the fight about Medicaid reveals that the Federal government is not doing a very good job with Medicaid? Apparently not.
To paraphrase the Apostle Paul, whether something is lawful is different from whether something is beneficial, and whether Medicaid, as currently implemented, is lawful is different from whether it is ethical or just or commendable or excellent.
The Founding Fathers would agree that a Federal “Medicaid for all” program that provided the same benefit to every American who met a standard eligibility criteria was a valid exercise of the Spending Clause and harmonious with the Tenth and Fourteenth Amendments. Given the courage demonstrated by the Founding Fathers in creating a country out of whole cloth, they might wonder why Congress lacks the courage to provide healthcare for America’s most vulnerable citizens that is equal for all.