It is well established that the maternal mortality rate in the U.S. is a stark outlier to other high-income countries, particularly for Black populations. The overall U.S. maternal mortality rate is 23.8 per 100K, as compared to 6.5 per 100K in the U.K. and 2.7 per 100K in Japan. Even worse, the maternal mortality rate in the U.S. for Black populations is 55.3 per 100K, a rate that is significantly higher than countries like Cuba, Mongolia and Syria.1,2,3
Additionally, over 40% of U.S. births are covered by Medicaid, reaching as high as 60% of births in states with lowest per capita income like Louisiana and Mississippi.4,5 As a result, state Medicaid programs have a significant role to play in reducing the U.S. maternal mortality rate, particularly among Black women, given the distressingly high maternal mortality rate for Black women and the disproportionate representation of the Black population in the non-elderly Medicaid population.6,7
Background
The White House has demonstrated its focus on improving maternal health outcomes by publishing the Biden-Harris Maternal Health Blueprint.8,9,10 In order for federal and state agencies to improve prenatal, delivery and postpartum care in Medicaid, measurement and benchmarking across a broad set of outcomes is essential, beginning with a detailed analysis of the causes of these well-documented adverse yet preventable outcomes.
Prior research has documented that certain outcomes are disproportionately worse for Medicaid births compared to commercial births. For example, in 2018 11.2% of Medicaid births were categorized as pre-term, compared to 9.1% of commercial births.11 Additionally, 9.8% of Medicaid births were characterized as low or very low birthweight, compared to 7.1% of commercial births. While a substantial amount of research is conducted by government agencies (CDC, HHS) and published in academic journals, issues of data recency, data obfuscation for privacy, limited geographic specification and incomplete representation of insurance coverage types inhibit analysis of Medicaid births. In this analysis, we analyzed several critical maternal health outcomes in Medicaid using our all-payer claims database at a national level.
Analytic Approach
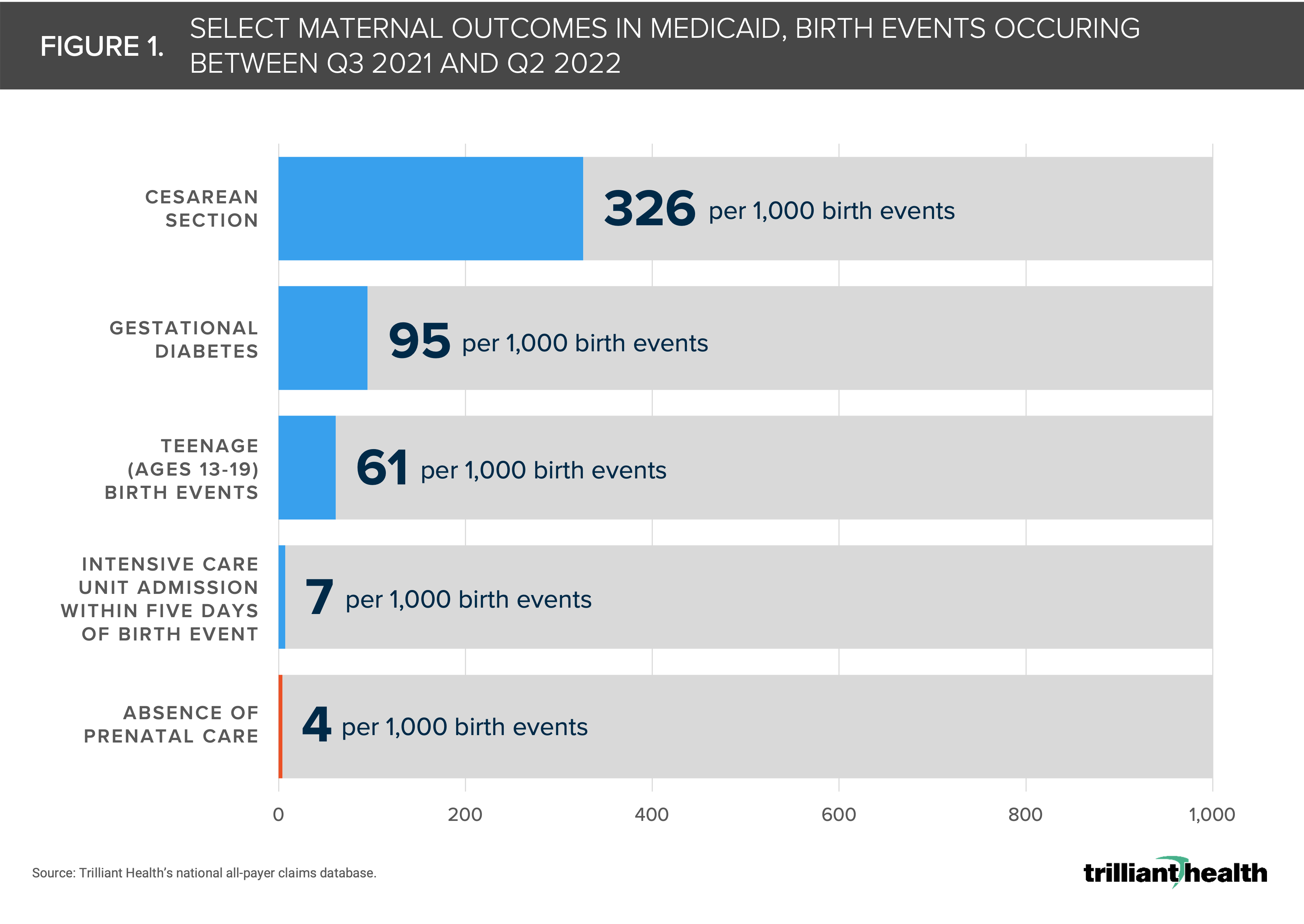
To analyze certain recent maternal outcomes in Medicaid, we studied births from Q3 2021 to Q2 2022, with a nine-month lookback period to analyze prenatal care. We limited our analysis to females ages 13 to 45 who were continuously enrolled in Medicaid for at least 12 months prior to birth. The outcomes we studied included Cesarean section rates, an absence of prenatal care preceding birth, postpartum ICU admissions, gestational diabetes, and teenage births (i.e., ages 13 to 19).
Findings
Of all Medicaid births taking place during the defined time period, 326 per 1,000 deliveries were Cesarean sections, aligning with the overall U.S. rate of 321 per 1,000. (Figure 1). While there is not a meaningful difference in Cesarean rates across pay types, the U.S. rate is notably higher compared to the global rate of 210 per 1,000.12,13 However, just 4 per 1,000 Medicaid births did not have any form of documented prenatal care. Although adherence to some form of prenatal care was strong in this population, the rate of teenage pregnancy was high (61 per 1,000), as was the rate of diagnosed gestational diabetes (95 per 1,000).